

Background: Radial tears of the meniscus represent a challenging clinical scenario because benign neglect and partial meniscectomy have both been shown to have negative biomechanical and long-term clinical consequences.
Hypothesis: Complex suture repair constructs have higher failure loads and stiffness values compared with simple constructs.
Study Design: Controlled laboratory study.
Methods: After radial transection of human cadaveric menisci, simulated tears were repaired arthroscopically by use of 1 of 4 repair constructs: (1) 2 inside-out horizontal sutures, (2) 2 all-inside horizontal sutures, (3) an all-inside Mason-Allen construct consisting of 4 sutures, or (4) an all-inside construct consisting of a figure-of-8 suture plus 1 horizontal suture. Meniscus specimens were harvested and tested to failure on an Instron machine. The Kruskal-Wallis test was used to evaluate for significance of maximal failure load and stiffness between groups.
Results: The mean maximum failure loads were 64 ± 20 N (inside-out horizontal construct), 75 ± 16 N (all-inside horizontal construct), 86 ± 19 N (Mason-Allen construct), and 113 ± 22 N (figure-of-8 plus horizontal construct). Interconstruct comparison revealed a statistically significant difference between the figure-of-8 plus horizontal construct and all 3 remaining constructs (P < .02) as well as the Mason-Allen construct when compared with the inside-out horizontal construct (P < .01). Statistical significance was not found between the all-inside horizontal construct and the Mason-Allen construct or between the all-inside horizontal construct and the inside-out horizontal construct (P = .2 and .7, respectively). Stiffness values were lower for the inside-out construct compared with the all-inside constructs (P < .05).
Conclusion: Complex all-inside repair constructs had significantly higher failure loads than a conventional, simple inside-out suture repair construct for repair of radial meniscal tears. Stiffness values among the all-inside groups were greater than those for the inside-out group.
Clinical Relevance: Arthroscopic techniques are presented to produce stronger radial meniscal tear repairs.
Keywords: meniscus; radial tear; repair; failure load
Eric A. Branch,* MS, Charles Milchteim,* MD, Bradley S. Aspey,* MD, Wei Liu,† PhD, Justin D. Saliman,‡ MD, and Adam W. Anz,*§ MDInvestigation performed at the Andrews Research and Education Institute, Gulf Breeze, Florida, USA
§Address correspondence to Adam W. Anz, MD, Andrews Research and Education Institute, 1040 Gulf Breeze Parkway, Gulf Breeze, FL 32561, USA (email: anz.adam.w@gmail.com).*Andrews Research and Education Institute, Gulf Breeze, Florida, USA.†Department of Kinesiology, College of Education, Auburn University, Auburn, Alabama, USA.‡Cedars-Sinai Orthopaedic Center, Los Angeles, California, USA.One or more of the authors has declared the following potential conflict of interest or source of funding: A.W.A. is a consultant for Ceterix Orthopaedics. J.D.S. is founder and chief medical officer for Ceterix Orthopaedics, holds a patent related to the suture-passing device used in the study, and is a consultant for Moximed. Funding for execution of this study was provided by Ceterix Orthopaedics.
The American Journal of Sports Medicine, Vol. 43, No. 9DOI: 10.1177/0363546515591994© 2015 The Author(s)
Radial tears of the meniscus may be more common than previously recognized. Studies in adults have suggested a 10% to 23% incidence of radial tear patterns,6,15,22 and a recent review of meniscal treatment in children and adolescents illustrated a 10% incidence.24 Biomechanical studies have established the negative consequences of leaving complete or near-complete radial tears untreated or treated with partial meniscectomy, demonstrating increased contact pressures and decreased contact areas at the surrounding articular surfaces in both scenarios.4,5,17,21 Retrospective and prospective studies have demonstrated that meniscal tears with a significant radial component are associated with a higher degree of meniscus extrusion and the development of osteoarthritis.2,12 A recent retrospective review illustrated decreased rates of osteoarthritis as well as increased functional scores in patients treated with meniscal repair compared with partial meniscectomy.25
Repair strength is important because it affects healing potential and rehabilitation protocols. Retrospective studies have described various repairs for radial meniscal tears involving central to peripheral needle penetration techniques that involve fixation within the perimeniscal capsule. These studied patterns include single suture horizontal, double suture horizontal, and crisscrossed transtibial constructs passed with outside-in, inside-out, and all-inside techniques.1,6,9,11,18,19,26,27 Four previous biomechanical studies have evaluated the failure load of radial repair constructs.3,10,13,16 All of these studies involved ex vivo suture placement and ex vivo tensile testing, with 3 studies involving porcine meniscus and 1 study involving human meniscus specimens. These studies illustrated that 2 horizontal sutures are better than 1 horizontal suture, a crossing suture pattern is superior to a parallel pattern, and an all-inside construct is likely stronger and stiffer than inside-out based constructs. However, these studies primarily evaluated simple suture patterns, and study is lacking on more complex suture patterns and suture repairs that are completely intrameniscal. Additionally, these previous studies evaluated constructs placed ex vivo without study of arthroscopically placed constructs.
The goal of this study was to compare the failure load and stiffness values of side-to-side all-inside arthroscopic suture patterns with values of previously described central to peripheral horizontal repair patterns. We evaluated 1 construct placed in a traditional inside-out fashion and 3 repair constructs, of increasing complexity, placed in an all-inside, intrameniscal fashion. Evaluation of the failure load and stiffness for different meniscal repair constructs will aid the clinician in decisions regarding optimal meniscal radial repair technique. We hypothesized that repair construct failure loads would vary based on suture construct design, postulating higher failure loads with increased repair technique complexity.
METHODS
A total of 50 menisci were used from 28 human cadaveric knee specimens. The mean specimen age was 57 ± 6 years (range, 42-63 years). Fifteen menisci were from female donors, and 35 menisci were from male donors. Ten menisci were used to establish a control group, tested intact without creating a radial tear. Five medial menisci and 5 lateral menisci were used for each group. We selected 10 specimens per group, as 8 specimens per group has proven to be a sufficient sample size in previous biomechanical in vitro studies on meniscus suture techniques.5,13 Additionally, upon power analysis, it was determined that a sample size of 10 specimens per study group would yield at least 80% power to detect the minimal between-group difference in maximum failure load of 27 N, assuming a nonparametric comparison of 4 groups, a group standard deviation of 20 N or less,9 and a type I error probability of .05.
Specimens were mounted to mimic a supine arthroscopic setup, with the knee free to move from 0° to 120°. Mounting the specimens involved exposing 3 inches of bone superior to the suprapatellar compartment and clamping in a 2-holed
specimen clamp. Holes were drilled through the bone once it was provisionally placed in the clamp and 2 metal rods were placed through the clamp and bone. In this simulated surgical position, varus and valgus stresses could be placed on the knee to open the medial and lateral compartments. Arthroscopic portals were created, and a diagnostic arthroscopy was performed. Specimens exhibiting macroscopic articular cartilage defects equal to or greater than Outerbridge 3 and/or meniscal degeneration or meniscal tears involving Cooper zones 0, 1, and/or 2 (ie, the peripheral two-thirds of the meniscus) were excluded from the study.7 Five menisci were excluded due to macroscopic degeneration upon initial arthroscopic evaluation.
A complete radial tear of the meniscus was created at the junction of the body and posterior horn (ie, at the junction of Cooper zones A and B on the medial meniscus and that of Cooper zones E and F on the lateral meniscus).7 Tear creation involved a percutaneous method using a scalpel with a No. 11 blade. Tears were created completely through the meniscal and capsular tissue. Although a radial tear involving the capsule is not a clinically common pattern, the capsule was included in tear creation to eliminate it as a confounding variable. Although not directly in the middle of the meniscus, the tear simulated a midbody radial tear of the meniscus. After tear creation, meniscal repair was performed arthroscopically. An arthroscopic suture-passing device (NovoStitch; Ceterix Orthopaedics) was used for the all-inside repairs, and typical long needles with zone-specific cannulas were used for the inside-out repair. The intrameniscal suture technique has previously been described.23 A No. 2-0 braided polyester and ultra–high-molecular-weight polyethylene suture (Fiberwire; Arthrex) was used for all repairs.
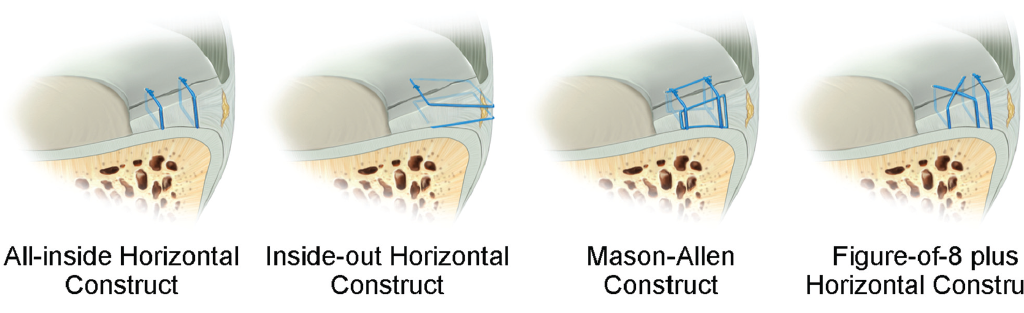
Four repair constructs were evaluated: 2 traditional horizontal sutures placed in an inside-out fashion (inside-out horizontal construct), 2 intrameniscal horizontal sutures placed in an all-inside fashion (all-inside horizontal construct), a Mason-Allen construct involving 4 sutures placed in an all-inside fashion (Mason-Allen construct), and an intrameniscal figure-of-8 suture plus a peripheral intrameniscal horizontal suture placed in an all-inside fashion (figure-of-8 plus horizontal construct) (Figure 1). All constructs used 2 sutures with the exception of the Mason-Allen construct, which involved 4 sutures: 2 stay sutures placed vertically and 2 suture loops placed horizontally. The inside-out horizontal construct included 1 horizontal suture on the femoral side and 1 on the tibial side.
Zone-specific cannulas and long needles loaded with No. 2-0 braided polyester and ultra–high-molecular-weight polyethylene suture (Fiberwire; Arthrex) were used to create the inside-out horizontal construct. A horizontal suture was placed on the femoral side of the meniscus, and 1 horizontal suture was placed on the tibial side of the meniscus. Punctures were placed approximately 5 mm from the periphery and 5 mm from the tear margin (Figure 2, A and B).
Creation of the all-inside horizontal construct involved passage of 1 end of a suture on 1 side of the tear approximately 3 mm from the periphery of the meniscus and 5 mm from the tear margin followed by passage of the other end of the suture on the other side of the tear approximately 3 mm from the periphery and 5 mm from the tear margin. The 2 ends were tied by use of standard arthroscopic Revo knots, involving 2 same-sided hitches followed by 3 alternating half hitches.14 A second horizontal suture was then placed in a similar fashion 8 mm from the periphery and tied (Figure 2, C and D). Creation of the Mason-Allen construct involved first placement of 1 vertical suture on each side of the tear approximately 5 mm from the tear. This involved passage of 1 end of a suture 3 mm from the periphery of the meniscus and 5 mm from the tear site. The opposite end of the suture was placed 8 mm from the periphery and 5 mm from the tear site. The 2 ends were tied. A similar vertical suture was placed on the opposite side of the tear.
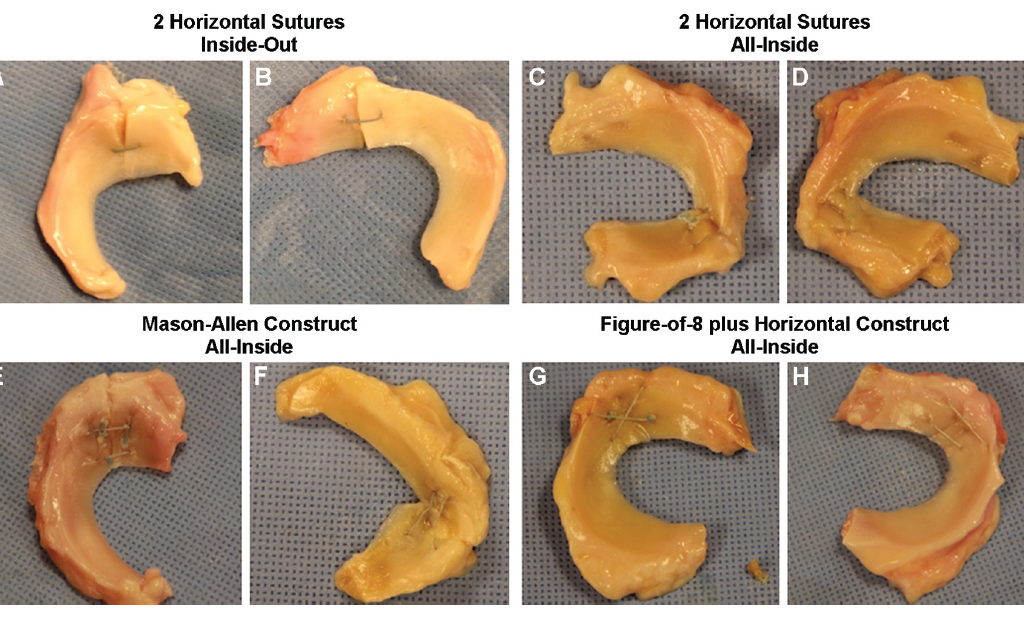
This was followed by placement of 2 horizontal sutures in a similar fashion to the intrameniscal horizontal sutures placed in an all-inside fashion construct, with each end of the suture passed on the far side of the vertical suture from the tear (Figure 2, E and F). Creation of the figure-of-8 plus horizontal construct involved 4 steps (see the online Video Supplement). The first step involved passing 1 free end of a suture (post) on the far side of the radial tear approximately 5 mm from the periphery of the meniscus. The second step involved passage of the opposite end of the suture (leading suture) approximately 5 mm from the periphery of the meniscus on the opposite side of the radial tear (near side) from the first passage. The third step involved passage of the leading suture through the central aspect of the meniscus, approximately 8 to 10 mm from the periphery, on the far side. The fourth step involved passage of the leading suture through the central aspect of the meniscus, approximately 8 to 10 mm from the periphery, on the near side (Figure 2, G and H). The post and leading end were tied, and a second horizontal suture was placed 3 mm from the periphery of the meniscus and tied. Knot tying for all sutures involved a Revo knot and a knot pusher.14
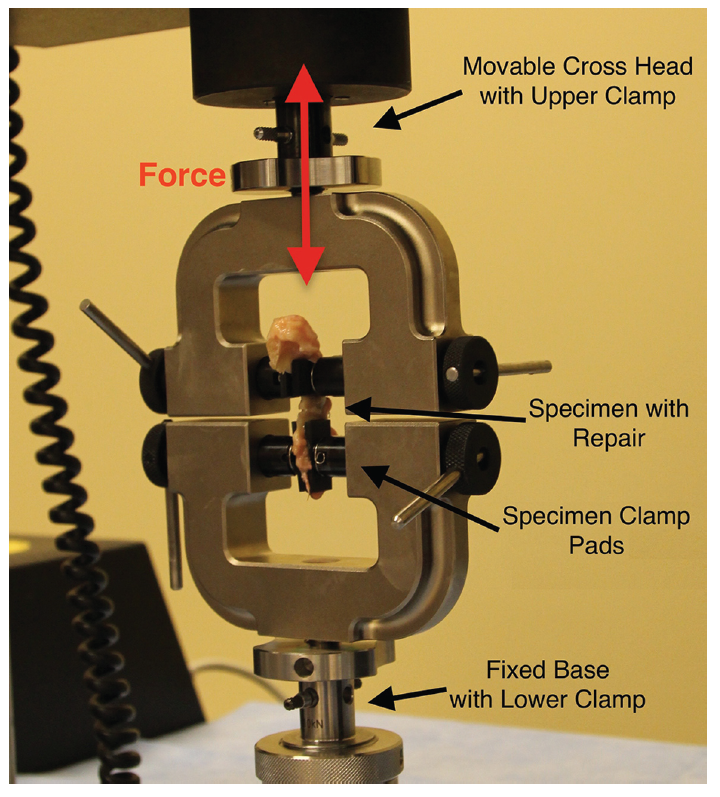
After arthroscopic placement of the repair constructs, the knees were disarticulated and the menisci were explanted by sharp dissection. Individual meniscus specimens were then tested to failure on a uniaxial material testing machine (Model 5565; Instron Corp) with 2 screw side-action grip specimen clamps (Model 2710-102). The screw side-action grip specimen clamps had a maximum load capacity of 500 N. Specimens were kept moist with saline solution and were tested within an hour of suture construct placement. Each specimen was initially mounted in the superior specimen mount in line with the circumferential fibers and lowered into the inferior specimen mount (Figure 3).
The tensile testing protocol included a preload period for 10 seconds, a preconditioning period with cyclic loading, and a period of load to failure. Throughout testing, tensile load and displacement were recorded at 10 Hz. The preconditioning period involved 20 cycles from 5 to 30 N at 0.5 mm/s, and the load to failure period involved an increase in force at a rate of 0.5 mm/s until failure. Throughout the entire testing process, actuator force and displacement were captured, and a displacement curve was generated by use of mechanical testing software (Bluehill 2; Instron Corp). Maximum failure load was defined as the first loss of structural integrity illustrated by the initial peak on the displacement curve. Stiffness values were determined by calculating the slope of the load-displacement curve during the initial loading of the construct from 5 to 30 N. The included region was linear and sufficiently below the failure load to ensure that nonlinear deformation was excluded. Meniscus specimens were kept moist before and during testing. Specimens were monitored for slippage within the clamp visually during testing as well as on post-test analysis of the displacement curve.
All data were checked for normality of distribution, and a Kruskal-Wallis 1-way analysis of variance by ranks was chosen to evaluate for statistical significance of maximum failure load and stiffness between groups, as the data were not distributed normally. Power calculations were done with simulations in SAS v 9.2 (SAS Institute Inc).
RESULTS
The control group exhibited the highest maximum failure load and stiffness values (Table 1). The figure-of-8 plus horizontal construct exhibited the highest maximum failure load among the repair constructs. The Mason-Allen construct exhibited the second highest failure load, followed by the all-inside horizontal constructs and the inside-out horizontal construct.
TABLE 1 Maximum Failure Load and Stiffness for Each Constructa
| TABLE 1 Maximum Failure Load and Stiffness for Each Constructa | ||
|---|---|---|
| Maximum Failure Load, N | Stiffness, N/mm | |
| Control group | 477 ± 144 | 37 ± 13 |
| Inside-out horizontal construct | 64 ± 20 | 8 ± 2 |
| All-inside horizontal construct | 75 ± 16 | 12 ± 3 |
| Mason-Allen construct | 86 ± 19 | 11 ± 2 |
| Figure-of-8 plus horizontal construct | 113 ± 22 | 11 ± 3 |
| aResults are reported as mean ± SD. | ||
Interconstruct comparison revealed statistical difference between the figure-of-8 plus horizontal construct and all 3 remaining constructs (P < .02) and the Mason-Allen construct when compared with inside-out horizontal construct (P < .01). Statistical significance was not found between the all-inside horizontal construct and the Mason-Allen construct (P = .2) or the inside-out horizontal construct (P = .7). Stiffness values of repair constructs were similar except that the inside-out horizontal construct had lower stiffness values than the other repair constructs (Table 1). For stiffness, interconstruct comparison revealed statistical difference between the inside-out horizontal construct and all 3 remaining constructs (P < .05). Statistical significance was not found between the all-inside horizontal, the Mason-Allen, and the figure-of-8 plus horizontal constructs. The failure mechanism for all specimens tested was meniscal tissue suture pull-through. Three specimens failed during the preconditioning cycle, and data for these 3 specimens were used in calculations. During control testing, 7 samples failed by slipping at the tissue clamp interface while 3 samples failed through elongation and tissue rupture; data for all specimens were used in calculations.
DISCUSSION
This study evaluated 4 suture constructs for radial meniscal tear repair: 3 intrameniscal repair constructs with all-inside arthroscopic technique and 1 repair construct using traditional inside-out technique for comparison. The strongest construct involved the most complex pattern of suture repair and had a mean maximum failure load of 113 N. Constructs illustrated low maximum failure loads when compared with a control group of intact menisci. The 2 complex, all-inside radial repair constructs were significantly stronger than a conventional inside-out repair construct, and all 3 all-inside repair constructs were stiffer than the inside-out construct. Previous biomechanical studies on radial repair have focused on optimizing simple central to peripheral suture placement; sutures have been placed ex vivo and then evaluated with similar biomechanical testing as used in this study.3,10,13,16 Herbort et al10 used porcine menisci, cyclic loading from 5 to 20 N 1000 times, and maximum failure load to compare double horizontal suture patterns to single suture patterns. Sutures were placed ex vivo and tied on the rim of the menisci, creating an inside-out style of repair constructs. The double horizontal pattern illustrated a significantly higher maximal failure load and significantly lower displacement compared with a single horizontal pattern. Additionally, constructs closer to the meniscal periphery performed significantly better than constructs placed centrally in the meniscus, while distance of suture placement from tear edge had no influence on construct performance. While the study by Herbort et al guides optimization of parallel horizontal suture for inside-out repair, Matsubara et al16 theorized that a crossed suture construct would capture a greater proportion of the semicircular-oriented meniscal collagen fibers and thus perform better than a simple horizontal construct in inside-out repair. Their study used fresh human menisci harvested during total knee arthroplasty, cyclic loading from 5 to 30 N 500 times, and 40 specimens with a mean specimen age of 76 years. The 2 simple sutures in a crossed pattern performed superiorly with a failure load of 78.96 ± 19.27 N and a stiffness of 8.01 ± 1.54 N/mm compared with the simple sutures in a parallel horizontal pattern with a failure load of 68.16 ± 12.92 N and a stiffness of 6.46 ± 1.12 N/mm. In our study we chose to use inside-out sutures in a horizontal fashion so that we could place 1 suture on the superior (femoral) surface and 1 suture on the inferior (tibial) surface as may be done when attempting to achieve anatomic reduction and uniform compression with traditional techniques. This was the most relevant pattern for comparison because the all-inside intrameniscal sutures inherently reduce and compress the femoral and tibial sides of the tear simultaneously and evenly.
Lee et al13 sought to compare an all-inside repair to an inside-out repair. Using porcine specimens, cyclic loading, and load to failure, the investigators found no significant difference between displacement, gapping, stiffness, or load to failure between 2 horizontal No. 2-0 sutures tied peripherally and an all-inside construct using a continuous suture and planches for peripheral security. The all-inside construct design also created an oblique arm between horizontal components of the repair. The all-inside group illustrated a maximum failure load of 86.2 ± 16.7 N and the inside-out group illustrated a maximum failure load of 89.8 ± 18.9 N. In a porcine model, Beamer et al3 compared 1 traditional inside-out suture to 1 side-to-side intrameniscal suture using the same device as in this study. Similar to the results of this present study, the ultimate failure load and stiffness were greater for the all-inside repairs. The investigators also found that the all-inside repair had less displacement after cyclic loading than the inside-out repair. Interstudy comparison is difficult considering porcine versus human tissue. Additionally, biomechanical testing protocols between studies differed, making direct comparisons difficult.
Previous biomechanical studies have investigated the integrity of the circumferential collagen fibrils and subsequent changes in contact pressure and areas.4,21 Bedi et al4 evaluated radial tears and repair of the medial meniscus in a cadaveric dynamic gait model. Radial tears involving up to 60% of the meniscus width did not illustrate a significant increase in contact pressure. Radial tears involving 90% of the meniscus resulted in altered contact mechanics but did not significantly alter peak and mean pressures; contact mechanics were not restored with a double horizontal inside-out repair. Partial meniscectomy of 90% tears resulted in an increase in peak and mean contact pressures as well as altered mechanics, suggesting that retained meniscal tissue in scenarios of tearing may provide some load transmission.4 Radial tears of the lateral meniscus have shown similar findings, with tears up to 60% having little effect on contact pressures and areas.5 However, 90% tears of the lateral meniscus illustrated significant increases in peak pressure and decreases in contact area, which were significantly improved with repair. Partial lateral meniscectomy revealed pressures and contact areas similar to 90% tears.5 A similar study using axial compression revealed near normal biomechanics with tears up to 75%, while tears involving 100% illustrated increases in contact pressure and decreases in contact area.21 Pressures and areas were significantly worse after complete meniscectomy. Repair with 2 horizontal sutures in an all-inside and repair with 2 horizontal sutures in an inside-out fashion resulted in restored contact pressures and improved contact areas.21 Assimilation of biomechanical studies suggests that complete radial tears should be pursued with repair, while tears 75% or less may do well with observation alone, as retained tissue appears to help retain normal biomechanics. This is tempered by a recent study illustrating good healing rates of longitudinal meniscal tears within the red-white zone.8 As techniques for repair continue to improve and further outcome data after repair are collected, indications for repair versus observation will further be refined.
Because a stiffer radial repair construct would theoretically resist gap formation while healing, the higher stiffness of the side-to-side repair groups as compared with the traditional inside-out repair group is notable. This study measured displacement and calculated stiffness based on actuator data from the mechanical testing machine. Although a previous study has used this method to determine displacement and stiffness, this method may lack exact displacement data.8 Within the repair groups, specimen slipping within the clamp was not observed. If not detected visually during testing, displacement through specimen slipping would have been evident on the force-displacement curve. The control group illustrated slipping in 7 of 10 specimens, suggesting that the true maximum failure load was higher than what could be measured with this testing design. However, the control group provided a benchmark for comparison of repair constructs to intact menisci in this testing design. Measuring displacement with markers and high-speed cameras could theoretically improve the testing model; however, this proved beyond the capabilities of our laboratory.
This study did not completely reproduce the natural loads and stresses of the meniscus after radial tear repair. Forces applied were uniaxial, while natural knee motion and loading produce vertical shear, radial extrusion, and axial compression. While the presented ex vivo comparison gives comparative insight between meniscal radial repair constructs, it does not effectively determine the ability of these constructs to restore normal meniscus biomechanics or the effects of the complex suture pattern on meniscal kinematics and physiologic characteristics. Further in vivo study would aid in the analysis of in vivo stresses as well as contact areas and pressures. While an in vivo study would better capture restoration of contact pressures and areas, the aim of this study was to compare the strength of different meniscal repair constructs in a simple and reproducible fashion.
A weakness of this study is the use of middle-aged cadaveric specimens (average age, 57 years; range, 42-63 years), in which meniscal repair is seldom indicated. The age of the specimens is difficult to control, as specimens younger than 40 years are not readily available. An additional weakness is the use of both medial and lateral meniscal tissue in each group, as this is a confounding variable. An additional limitation of the biomechanical testing is the lack of displacement data. This study design was kept simple for comparison of failure load and stiffness of suture construct to evaluate more meniscal constructs.
Biomechanical testing of meniscal repair is also limited as it represents meniscal repair construct strength at time point zero only. The strength of healing tissue cannot be accounted for in cadaver study and should be considered when meniscal repair is contemplated. On several specimens, a medial collateral ligament (MCL) release was required for access to the posterior medial horn. While specimens that had articular cartilage defects equal to or greater than Outerbridge 3 were excluded, the majority of the specimens represented an older population with many specimens including Outerbridge 1/2 changes. For these cases, release of the superficial MCL was often required. While in clinical practice a superficial MCL release may have limited consequence, biomechanical studies have suggested that incomplete radial tears of the medial meniscus may have limited effect, and clinicians should consider this in deciding when to repair a radial tear. In this scenario, use of the repair device has been manageable.
In conclusion, this in vitro study found that the failure loads of the 2 complex, all-inside radial repair constructs were significantly higher than a conventional inside-out repair construct. The figure-of-8 construct resulted in the highest failure load. Additionally, all 3 all-inside repair constructs were stiffer than the inside-out construct.
A Video Supplement for this article is available in the online version or at http://ajsm.sagepub.com/supplemental.
REFERENCES
- Anderson L, Watts M, Shapter O, et al. Repair of radial tears and posterior horn detachments of the lateral meniscus: minimum 2-year follow-up. Arthroscopy. 2010;26(12 ):1625-1632.
- Badlani JT, Borrero C, Golla S, Harner CD, Irrgang JJ. The effects of meniscus injury on the development of knee osteoarthritis: data from the osteoarthritis initiative. Am J Sports Med. 2013;41(6):1238-1244.
- Beamer BS, Masoudi A, Walley KC, et al. Analysis of a new all-inside versus inside-out technique for repairing radial meniscal tears. Arthroscopy. 2015;31(2):293-298.
- Bedi A, Kelly NH, Baad M, et al. Dynamic contact mechanics of the medial meniscus as a function of radial tear, repair and partial meniscectomy. J Bone Joint Surg Am. 2010;92(6):1398-1408.
- Bedi A, Kelly NH, Baad M, et al. Dynamic contact mechanics of radial tears of the lateral meniscus: implications for treatment. Arthroscopy. 2012;28(3):372-381.
- Choi CJ, Choi YJ, Song IB, Choi CH. Characteristics of radial tears in the posterior horn of the medial meniscus compared to horizontal tears. Clin Orthop Surg. 2011;3(2):128-132.
- Cooper DE, Arnoczky SP, Warren RF. Meniscal repair. Clin Sports Med. 1991;10:529-548.
- Feucht MJ, Grande E, Brunhuber J, Burgkart R, Imhoff AB, Braun S. Biomechanical evaluation of different suture techniques for arthroscopic transtibial pull-out repair of posterior medial meniscus root tears. Am J Sports Med. 2013;41(12):2784-2790.
- Haklar U, Kocaoglu B, Nalbantoglu U, Tuzuner T, Guven O. Arthroscopic repair of radial lateral meniscus tear by double horizontal sutures with inside-outside technique. Knee. 2008;15(5):355-359.
- Herbort M, Siam S, Lenschow S, Petersen W, Zantop T. Strategies for repair of radial tears close to the meniscal rim: biomechanical analysis with a cyclic loading protocol. Am J Sports Med. 2010;38(11):2281-2287.
- James EW, LaPrade CM, Feagin JA, LaPrade RF. Repair of a complete radial tear in the midbody of the medial meniscus using a novel crisscross suture transtibial tunnel surgical technique: a case report [published online June 3, 2014]. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3089-z.
- Lee DH, Lee BS, Kim JM, et al. Predictors of degenerative medial meniscus extrusion: radial component and knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):222-229.
- Lee YH, Nyland J, Burden R, Caborn DN. Cyclic test comparison of all-inside device and inside-out sutures for radial meniscus lesion repair: an in vitro porcine study. Arthroscopy. 2012;28(12):1873-1881.
- Loutzenheiser TD, Harryman DT, Ziegler DW, Yung SW. Optimizing arthroscopic knots using braided or monofilament suture. Arthroscopy. 1998;14(1):57-65.
- Magee T, Shapiro M, Williams D. MR accuracy and arthroscopic incidence of meniscal radial tears. Skeletal Radiol. 2002;31(12):686-689.
- Matsubara H, Okazaki K, Izawa T, et al. New suture method for radial tears of the meniscus: biomechanical analysis of cross-suture and double horizontal suture techniques using cyclic load testing. Am J Sports Med. 2012;40(2):414-418.
- Mononen ME, Jurvelin JS, Korhonen RK. Effects of radial tears and partial meniscectomy of lateral meniscus on the knee joint mechanics during the stance phase of the gait cycle—a 3d finite element study. J Orthop Res. 2013;31(8):1208-1217.
- Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscus tears extending into the avascular zone with or without anterior cruciate
- ligament reconstruction in patients 40 years of age and older. Arthroscopy. 2000;16(8):822-829.
- Noyes FR, Barber-Westin SD. Arthroscopic repair of meniscal tears extending into the avascular zone in patients younger than twenty years of age. Am J Sports Med. 2002;30(4):589-600.
- Noyes FR, Barber-Westin SD. Clinical healing rates of meniscus repairs of tears in the central-third (red-white) zone. Arthroscopy. 2014;30(1):134-146.
- Ode GE, Van Thiel GS, McArthur SA, et al. Effects of serial sectioning and repair of radial tears in the lateral meniscus. Am J Sports Med. 2012;40(8):1863-1870.
- Ozcok G, Circi E, Gonc U, Irgit K, Pourbagher A, Tandogan RN. Radial tears in the root of the posterior horn of the medial meniscus. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):849-854.
- Saliman JD. The circumferential compression stitch for meniscus repair. Arthrosc Tech. 2013;2(3):e257-e264.
- Shieh A, Bastrom T, Roocroft J, Edmonds EW, Pennock AT. Meniscus tear patterns in relation to skeletal immaturity: children versus adolescents. Am J Sports Med. 2013;41(12):2779-2783.
- Stein T, Mehling AP, Welsch F, Eisenhart-Roth RV, Jager A. Long-term outcome after arthroscopic meniscal repair versus arthroscopic partial meniscectomy for traumatic meniscal tears. Am J Sports Med. 2010;38(8):1542-1548.
- Van Trommel MF, Simonian PT, Potter HG, Wickiewicz TL. Arthroscopic meniscal repair with fibrin clot of complete radial tears of the lateral meniscus in the avascular zone. Arthroscopy. 1998;14(4):360-365.
- Yoo JC, Ahn JH, Lee SH, Kim JH. Suturing complete radial tears of the lateral meniscus. Arthroscopy. 2007;23(11):1249.e1-1249.e7.
For additional information on ACL knee injuries, or to learn more about what is involved during ACL reconstruction surgery, please contact the office of orthopedic knee surgeon, Dr. Adam Anz, serving the greater Pensacola, Gulf Breeze, and Gulf Coast communities.


