

Abstract
Objectives:
This scoping review aims to evaluate the safety and efficacy of orthobiologics in theTreatment of Greater Trochanteric Pain Syndrome (GTPS), with a focus on pain relief, functional improvement, and quality of life.Methods:
We conducted a comprehensive search of PubMed, Embase, Cochrane Library, Web of Science, Scopus, Google Scholar, and CINAHL for studies published from January 1, 2000, to March 20, 2024. Eligible studies included case series, cohort studies, case-control studies, and randomized controlled trials (RCTs) that investigated the use of orthobiologics for GTPS. The primary outcomes assessed were pain, function, and quality of life. The quality of the studies was evaluated using the JADAD scale, the Cochrane Risk of Bias Tool, and the MINORS score.Results:
The review included 19 studies involving a total of 811 participants. Platelet-rich plasma (PRP) was found to significantly reduce pain, as measured by the VAS scores, and to improve functional outcomes including the modified Harris Hip Score (mHHS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores. These findings suggest that PRP may be an effective treatment for GTPS. The studies reported minimal side effects that were generally mild and transient.Conclusion:
PRP and other orthobiologic treatments show promise in managing GTPS, showing good safety profiles and potential benefits. However, further high-quality RCTs are necessary to confirm long-term efficacy and to establish standardized treatment protocols.Level of evidence: II
Introduction
Greater Trochanteric Pain Syndrome (GTPS) is a musculoskeletal condition characterized by pain in the lateral hip area.1 It commonly affects older adults, particularly middle-aged women,2,3 with approximately 1 in 4 women over the age of 50 experiencing this condition.4 Annually, GTPS impacts around 1.8 per 1,000 individuals5 and is most prevalent during the fifth and sixth decades of life.4 GTPS includes conditions such as trochanteric bursitis, gluteal tendinopathy, and coxa saltans.6,7 These associated disorders can exhibit varying clinical features, which contribute to the complexity of diagnosis and treatment. Additionally, GTPS is often linked with other musculoskeletal conditions, such as osteoarthritis and lower back pain,6 which further complicate its management and may adversely affect treatment outcomes.1,4 Management of GTPS typically begins with conservative treatments including nonsteroidal anti-inflammatory drugs (NSAIDs), weight management, and targeted strengthening exercises for the gluteal muscles.8,9 When these measures fail to provide adequate relief, more intensive treatments, such as corticosteroid injections (CSI) or, in severe cases, surgical interventions may be necessary. Injections, including corticosteroids or orthobiologic options, are generally considered when patients continue to experience significant pain and restricted movement after attempting conservative treatments, which may include NSAIDs, physical therapy, and lifestyle modifications.10,11 They are typically recommended when pain persists and interferes with daily activities, and initial non-surgical approaches do not yield sufficient relief.8 While corticosteroids can offer short-term pain relief, their long-term effectiveness is limited, underscoring the need for alternative and more sustainable treatment options.12
———-
Research performed at Mashhad University of Medical Sciences, Mashhad, Iran
Received: 18 September 2024
Accepted: 20 November 2024
Keywords:
Autologous tenocyte injection, Bone marrow aspirate concentrate, Corticosteroid injection, Greater trochanteric pain syndrome, Hyaluronic acid, Orthobiologics, Platelet-rich plasma, Scoping Reviewhttp://abjs.mums.ac.ir
Email: m.ghorbani96@gmail.com/ Ghorbani.m@aol.com
Noncommercial 4.0 International License
https://creativecommons.org/licenses/by-nc/4.0/deed.en
Orthobiologics, derived from sources such as bone marrow and blood, are being studied for their potential effects on musculoskeletal repair.10,13 These substances contain cytokines and growth factors that, when injected, target the treatment area to support healing, reduce inflammation, and repair tendons, bones, ligaments, and muscles.14-17 Common orthobiologics include platelet-rich plasma (PRP),18 bone marrow aspirate concentrate (BMAC),18,19 bone morphogenetic proteins,10,16 mesenchymal stem cells,10 hyaluronic acid (HA),20 autologous tenocyte injection (ATI),21 and amniotic membrane.10 PRP and BMAC have gained the most attention for their role in promoting tissue healing and reducing inflammation.18,22 while HA and ATI have also shown promising results.20,21 Orthobiologics are also used in hand surgery, foot and ankle fusion, and hip disorders to promote bone healing and joint stability.14,17,23
Despite the potential benefits of orthobiologics, significant challenges persist, including variability in preparation, administration, and clinical outcomes. These factors complicates the establishment of standardized treatment protocols. Existing studies on these treatments often vary in methodology and quality, relying on small sample sizes or retrospective data. This variability complicates comprehensive assessments of their effectiveness and cost-efficiency.4,10,14,15 This scoping review focuses on chronic GTPS and aims to provide an overview of the current evidence regarding the safety and efficacy of orthobiologic treatments. Additionally, this review will identify gaps in the existing research, emphasizing areas where further studies are needed to optimize the use of these promising therapies.
Materials and Methods
Search Strategy
Search databases including PubMed, Embase, Cochrane Library, Web of Science, Scopus, Google Scholar, and CINAHL were searched using PRISMA principles. Using a combination of terms associated with GTPS and orthobiologics therapies, the search covered the period from January 1st, 2000 to March 20th, 2024. The search terms were modified to fit the particular indexing system of each database. The objective was to document how orthobiologic therapy improved over a 20-year period. A comprehensive strategy for each database is detailed in Appendix A. Using a PRISMA flow diagram, we presented the number of records obtained from each database, along with the selection process.
Study Screening
Two reviewers utilized Covidence software to independently screen the abstracts and titles. To ensure consistency, a calibration procedure was conducted earlier. Subsequently, each full text was evaluated independently, and any discrepancies were settled by consensus or by involving a third reviewer. If feasible, non-English studies were translated, and attempts were made to obtain full-text papers through interlibrary loans or direct communication with the authors.Inclusion and Exclusion Criteria
Studies that met the following criteria were included: (1) randomized controlled trials (RCTs), cohort studies, case-control studies, or case reports; (2) clinical outcomes, functional assessments, quality of life (QoL) metrics, and other results reported from patients with GTPS, bursitis, or gluteal tendinopathy after using PRP, BMAC, or any other biologic product.
Studies were excluded if they met any of the following criteria: (1) Inaccessible, missing data, or a full-reported article was not available; (2) focused solely on surgical interventions or reported outcomes exclusively from post-surgical patients; (3) included patients with a history of surgery for GTPS, unless treated exclusively with non-surgical methods; (4) duplicates, studies with weak scientific methodology, conference presentations, reviews, editorials, comments, and publications that were not peer-reviewed (e.g., dissertations); (5) missing outcomes of interest.
Quality Assessment
We assessed the quality of RCTs using the Cochrane Risk of Bias Tool and the JADAD scale. The JADAD scale, which has a maximum score of five, evaluates studies based on three key aspects: randomization, blinding, and participant withdrawals. Studies that scored three or above were considered to be of high quality. The Cochrane Risk of Bias Tool examines six types of bias: selection bias, performance bias, detection bias, attrition bias, reporting bias, and other potential sources of bias.
For non-randomized studies, we utilized the 2015 update of the Methodological Index for Non-Randomized Studies score (MINORS). This tool has a maximum score of 24 for comparative studies and 16 for non-comparative studies, encompassing 12 items (8 for non-comparative studies and 4 additional for comparative studies). Studies were classified as high quality if they achieved a score of 12 or higher for non-comparative studies and 18 or higher for comparative studies.
Results
Study Selection
There were 518 possibly related citations found in the initial search. 387 studies were excluded for not meeting the eligibility requirements. After 68 duplicates were excluded, the titles and abstracts of the 450 remaining studies were reviewed. 39 studies were excluded for various reasons after the full texts of the remaining 63 papers were evaluated. In the end, 811 participants from 19 trials were included in the scoping review. The PRISMA flow diagram details on the study selection process [Figure 1].
Study Characteristics
With 811 individuals, the study comprised 11 RCTs, 1 prospective cohort study, 7 case series, and 1 case report. Of the participants, 79.5% were female, with a mean age of 56.5 years. Injections of corticosteroids, HA, ATI, PRP, BMAC, and placebos were among the interventions used [Tables 1-3].
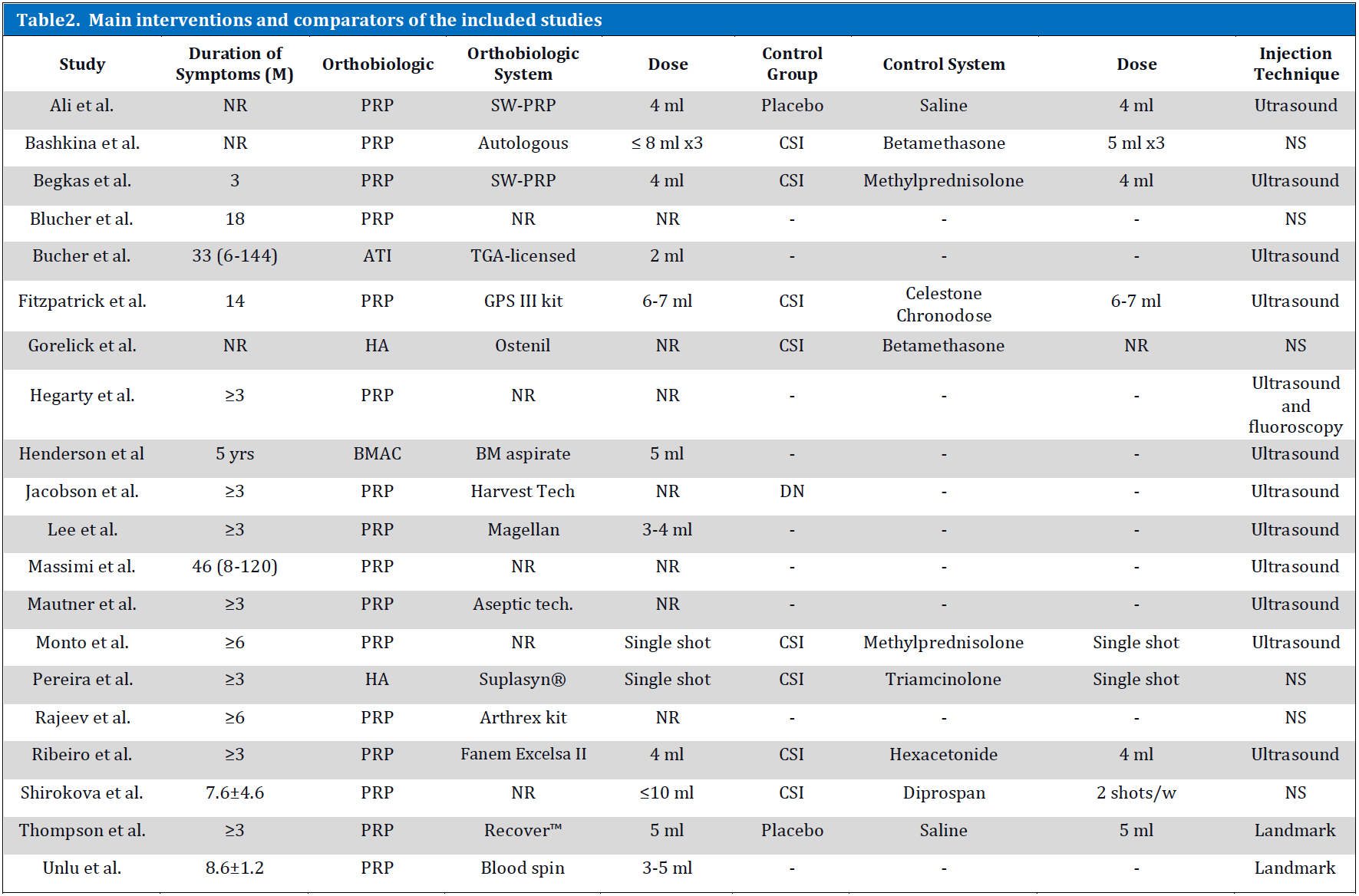
Interventions and Comparators
Various orthobiologic systems, such as the GPS III kit and SW-PRP, were utilized to administer PRP, indicating a variety of preparation techniques. The administered doses ranged from 2 ml to 10 ml, indicating various treatment modalities. A placebo, consisting of saline or CSI, was frequently administered to the control groups. While fluoroscopy or landmark approaches were used in some trials, ultrasound guidance was used predominantly in most injection techniques to ensure the precise delivery of the treatment [Table 2].
Outcome Assessments
Using a variety of patient-reported outcome measures (PROMs), the most frequently examined outcomes were pain and function. Pain evaluation was mostly carried out utilizing the Visual Analogue Scale (VAS), the Numeric Rating Scale (NRS), and Palpatory Tenderness (PT) across the majority of orthobiologic therapy trials. The Harris Hip Score (HHS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) were often used to assess functional outcomes. Limited number of studies assessed QoL; two of these studies used the International Hip Outcome Tool (iHOT-12 and iHOT-33) [Table 3].
Quality Assessment
Depending on the study design, the quality of the included studies varied. Based on the JADAD scale, the quality scores of the RCTs were generally higher, ranging from 3 to 5, in contrast, the non-randomized studies received MINORS ratings that ranged from 10 to 20, with majority scoring between 14 and 16 [Table 4].
Systematic Outcome Assessments
This scoping review included a variety of studies that examine the efficacy and safety of various orthobiologic treatments for managing chronic GTPS. The primary interventions studied included PRP, BMAC, HA, and ATI. Below, we present the findings categorized by intervention type, highlighting pain relief, functional improvement, and quality of life outcomes, while drawing comparisons to emphasize trends and variations across the studies.
Most main studies have compared PRP to CSI, which are commonly used in clinical practice for short-term relief. Across these studies, PRP consistently showed promising results for long-term pain management and functional improvement, although short-term outcomes occasionally favored CSI. Limited data are available for BMAC, HA, and ATI with most insights drawn from case studies and small trials. However, these reports underscore the potential as regenerative therapies.
| Table 1. Main demographic characteristics of the included studies | ||||||||
|---|---|---|---|---|---|---|---|---|
| Study | Country | Year | Study Design | Mean Age (SD) | Patient NO | Female (%) | Orthobiologics | Diagnosis Criteria |
| Ali et al. | UK | 2021 | RCT | 57.5 (NR) | 64 | 56 (87.5) | PRP | Clinical |
| Bashkina et al. | Russia | 2011 | RCT | 58.55 (8.1) | 40 | 40 (100) | PRP | Clinical |
| Begkas et al. | Greece | 2020 | RCT | 48.7 (NR) | 24 | 18 (75) | PRP | Clinical |
| Blucher et al. | UK | 2016 | CS | 60 (NR) | 85 | 68 (80) | PRP | Clinical |
| Bucher et al. | Australia | 2017 | CS | 52.25 (8.78) | 12 | 12 (100) | ATI | Clinical |
Orthobiologics and Pain
PRP vs CSI:PRP has been compared with CSI in several studies. Bashkina et al.24 study involving 71 patients reported a statistically significant decrease in the VAS pain intensity score in the PRP group at one, three, and six months post-intervention. Begkas et al.25 conducted a randomized clinical trial with 24 patients, finding no significant differences in pre-injection VAS score between the PRP and CSI groups; however the PRP group showed a significant reduction in pain (P < 0.05). Monto et al.26 trial with 40 participants found a significant improvement in WOMAC scores for the PRP group (P = 0.001), indicating superior pain relief compared to CSI. Shirokova et al.27 reported that PRP significantly reduced pain over six months, while CSI provided only short-term relief (P = 0.0001). However, Ribeiro et al.28 pilot study showed no significant difference in pain outcomes between PRP and CSI, although CSI exhibited a notable decrease in pain over time (P = 0.004).
PRP vs Placebo/ Dry Needling / No Control:
The efficacy of PRP without a comparative control has also been documented. Ali et al.29 randomized controlled trial with 80 patients that compared PRP to placebo (normal saline) found no statistically significant difference in the VAS scores at three months, despite improvements from baseline in both groups. Thompson et al.30 conducted a double-blind study showing that PRP did not significantly change pain levels compared to the placebo (P > 0.05). Jacobson et al.31 study compared PRP to tendon fenestration and found significant pain reduction in both groups, but no significant difference between the treatments (P = 0.16623). Blucher et al.32 and Massimi et al.33 reported significant pain reduction in PRP-treated patients (P < 0.05), although their studies lacked control groups for comparison. Mautner et al.34 multicenter retrospective analysis showed that 81% of patients experienced moderate to complete symptom relief following PRP injections. Unlu et al.35 reported a significant reduction in VAS scores from baseline to six weeks and six months in seven patients (P = 0.001). Hegarty et al.36 study involving seven women found a six-point improvement in VAS scores after PRP treatment. Rajeev et al.37 study observed a decline in VAS scores among 32 patients with severe GTPS following hip replacement; however they observed gradual increases in scores over time.
HA vs CSI:
Comparative studies on HA and corticosteroids have shown varied outcomes. Gorelick et al.38 retrospective study of 99 patients reported significant improvements for VAS score in both the HA and combination therapy groups when compared to the corticosteroid-only treatment. Initial pain relief was observed at six weeks, although VAS scores showed a slight increase at three and six months. Pereira et al.39 study of 40 patients indicated substantial reductions in VAS scores for both the HA and CSI groups at the 1-, 3-, and 6-month follow-ups (P < 0.001), with no significant difference between the two treatments.BMAC vs No Control:
Henderson et al.40 documented a significant reduction in pain in a 57-year-old female patient treated with BMAC. The VAS score decreased from 10 at baseline to 0.2 at six months, demonstrating a substantial 9.8-point reduction. This finding indicates the potential efficacy of BMAC for pain management in GTPS.ATI vs No Control: A prospective pilot study conducted by Bucher et al.21 involving patients with an average age of 52.8 (SD 8.4) years revealed a significant reduction in pain using ATI. The VAS scores improved notably within the first three months and continued to show progress up to 12 months, suggesting that ATI may be a promising treatment option for pain relief in GTPS.Orthobiologics and Function
PRP vs CSI: The comparison between PRP and CSI in terms of functional outcomes is well-documented. Bashkina et al.24 conducted a study evaluating functional status using the WOMAC index. This study showed that PRP consistently outperformed CSI at all follow-up periods, with improvements 2.33 and 2.98 times greater at three and six months, respectively. Similarly, Monto et al.26 randomized controlled trial involving 40 patients reported that the PRP group sustained improvements in HSS and WOMAC scores at 3, 6, and 12 months, while the CSI group exhibited initial gains followed by a decline (P < 0.001). These findings suggest that PRP may offer longer-lasting functional benefits compared to CSI.Begkas et al.25 clinical trial found that both the PRP and CSI groups showed significant improvement in post-treatment HHS; however PRP demonstrated the most pronounced improvement over time. Fitzpatrick et al.41 reinforced these findings in their study involving 80 patients, which revealed significant improvement in the mHHS (modified Harris Hip Score) within the PRP group, with 82% and 56.7% of patients meeting the Minimal Clinically Important Difference (MCID) at 12 weeks. Additionally, Shirokova et al.27 observed that PRP therapy resulted in a 20.8% increase in hip joint external rotation over six months, coupled with a lower Lequesne Index and improved functional outcomes, indicating PRP’s potential in minimizing disability associated with GTPS.However, the results were not universally favorable for PRP. Ribeiro et al.28 pilot study showed that although both the PRP and CSI groups experienced functional gains, the CSI group had a slight edge in WOMAC and HHS scores, particularly in short-term improvements. These results highlight that while PRP may provide better long-term outcomes, CSI can offer more immediate short-term relief.PRP vs Placebo/ Dry needling / No Control
The comparative effectiveness of PRP compared to placebo or dry needling has yielded mixed results. Ali et al.29 study involving 80 patients found that both the PRP and placebo groups experienced improvements in mHHS after three months although these differences were not statistically significant (P > 0.05). Despite a decline in scores at six months, the improvements remained above baseline values. Additionally, Lee et al.42 registry study noted that combining PRP with needle tenotomy led to significant functional improvements for patients with gluteus medius tendinopathy, as evidenced by enhanced Hip Outcome Score – Activities of Daily Living (HOS-ADL) and HOS-Sport scores. Massimi et al.33 retrospective case series involving 10 patients, which reported a significant functional improvement (P = 0.001) as measured by the Functional Rating Index (FRI). Rajeev et al.37 prospective study found significant increases in the median HHS three months following the PRP treatment. Nevertheless, the scores gradually declined at six months and one year, suggesting a potential waning of effects over time.HA vs CSI:
HA has been investigated as an alternative to CSI for functional improvement. In Gorelick et al.38 retrospective study, HA-treated patients showed marked improvement in Hip Disability and Osteoarthritis Outcome Score (HOOS) scores, increasing from a baseline mean of 27 (SD 4) to 66 (SD 2) at six months and 77 (SD 4) at one year (P < 0.05). Additionally, Pereira et al.20 comparative study using the Likert scale found significant functional gains in both the HA and CSI groups at 1-, 3-, and 6-month intervals, with no notable differences between the two treatments. Furthermore, high patient satisfaction was reported in the HA group, indicating its potential as a viable treatment option.BMAC vs No Control:
Limited evidence exists regarding impact of BMAC on functional outcomes; however Henderson et al.40 presented a compelling case report showing substantial improvement. The patient progressed from phase 7 (indicating the highest level of dysfunction) to phase 1 on the modified Nirschl Pain Phase Scale (mNPPS) within six months. Additionally, hip abductor strength improved from 3/5 to 4/5 by 12 weeks, accompanied by the resolution of Trendelenburg gait.ATI vs No Control:
In Bucher et al.’s 21 prospective pilot study, it was shown that ATI significantly improves functional outcomes. The Oxford Hip Score (OHS) increased by 8.3 points at six months (P = 0.009) and by 14.9 points at 12 months (P < 0.001). These results indicate that ATI holds promise for improving function over an extended duration.Orthobiologics and Quality of Life
PRP vs CSI:
Shirokova et al.27 study comparing PRP and CSI provided clear evidence that PRP was superior in enhancing QoL. The study revealed that patients treated with PRP consistently had lower scores on the Center for Epidemiologic Studies Depression Scale (CES-D), indicating a significant reduction in depressive symptoms and an overall improvement in QoL (P < 0.05). These findings underscore the potential of PRP not only for alleviating physical symptom s but also for its broader psychological and QoL benefits, suggesting a more comprehensive impact on patient well-being compared to CSI.PRP vs Placebo/ Dry Needling / No Control
The impact of PRP on QoL in the absence of a direct control group or when compared to alternative therapies, such as dry needling, was also explored. Blucher et al.32 demonstrated significant improvements in EuroQol 5-Dimension (EQ-5D) Utility scores, VAS ratings, and HOOS following PRP injections, indicating an enhancement in QoL. This suggests that PRP may positively influence both pain levels and overall QoL, offering benefits that extend beyond standard pain management. Similarly, Lee et al.42 registry study found significant improvements in iHOT-33 scores among 21 patients treated with PRP in combination with needle tenotomy, showing that this combined treatment was effective in improving functional performance and QoL over the follow-up period.HA vs CSI:
The study conducted by Gorelick et al.38 highlighted the efficacy of HA compared to CSI in improving QoL among patients with GTPS. Patients treated with HA showed substantial improvements in HOOS scores, rising from a baseline mean of 27 (SD 4) to 77 (SD 4) after one year (P < 0.05). These results emphasize HA’s potential as a viable alternative to corticosteroids for enhancing QoL in the long term. The significant year-long improvement noted in the HA group suggests that HA may provide sustainable benefits regarding patient QoL and functional outcome.BMAC vs No Control:
Although BMAC is less frequently studied, Henderson et al.40 provided a detailed case report showing substantial functional gains that indirectly indicated an enhanced QoL. The patient’s mobility and pain levels improved significantly by the six-month follow-up, likely contributing to a better QoL. However, direct measures of QoL were not reported, highlighting the need for more comprehensive studies that include specific QoL assessments to better understand the full impact of BMAC.ATI vs No Control:
Bucher et al.21 prospective pilot study on ATI provided promising data regarding improvements in on QoL. The study reported significant gains in the Physical Component Summary (PCS) subscale of the Short Form-36 (SF-36), with mean scores increasing by 15.2 points from baseline to 12 months (P < 0.001), and further increasing by an average of 12.8 points at 24 months (P < 0.001). These results indicate that ATI not only facilitates physical recovery but also contributes to sustained improvements in patients’ QoL over extended periods.Orthobiologicss and Adverse Events
PRP:
Adverse events related to PRP injections were generally mild and transient. The most common issue reported was pain at the injection site, which usually resolved within a few days without major complications. For example, Begkas et al.25 reported that 70.8% of patients (17 out of 24) experienced injection site pain lasting approximately three days, with no severe adverse effects noted. Similarly, Lee et al. observed temporary post-treatment soreness that was self-limiting. Fitzpatrick et al. found minor soreness within 48 hours after PRP treatment during a 12-week rehabilitation program, but no significant adverse events were reported. Ribeiro et al.28 and Unlu et al.35 confirmed PRP’s safety, with no cases of infection, muscle or tendon rupture, or serious complications.HA:
Studies involving HA treatments have also showed minimal adverse events. In Gorelick et al.38 study, no significant side effects were reported, highlighting HA as a well-tolerated treatment option. Similarly, Pereira et al.20 noted no secondary adverse effects in their comparative study, emphasizing HA’s safety profile, especially for patients who are contraindicated for CSI, such as those with diabetes mellitus.BMAC:
Henderson et al.40 reported no complications following BMAC treatment in a 57-year-old patient. The injection was well tolerated, with no adverse events noted during the follow-up period. This finding supports the potential safety of BMAC in managing musculoskeletal conditions.ATI:
Bucher et al.21 found minimal adverse effects in their study on ATI. Three patients experienced immediate discomfort at the biopsy site, which was effectively managed with NSAIDs and resolved without further complications. No serious complications were reported; however one patient with prolonged symptoms ultimately required surgical intervention after 12 months, although this was unrelated to the safety of ATI.Synthesis of Findings
Orthobiologic treatments, such as PRP, HA, BMAC, and ATI have shown different levels of success in treating chronic GTPS, particularly in terms of pain relief, functional improvement, and QoL. PRP has consistently showed good results for long-term pain relief and functional enhancement, often outperforming CSI, as evidenced by studies conducted by Bashkina et al.24 and Monto et al.26 While CSI may offer quicker pain relief, PRP provides more lasting benefits. HA also showed positive effects, with study by Gorelick et al.38 showing significant improvements in pain and function over one-year period, establishing it as a solid non-steroidal option. BMAC, highlighted in Henderson et al.40 case report, showed promise with marked pain reduction and function gains; however further extensive research is needed. In addition, ATI has shown positive results, with Bucher et al.21 reporting significant functional improvements and QoL benefits lasting up to two years.QoL positive outcomes were notable with PRP and ATI. Shirokova et al.27 found that PRP reduced depressive symptoms and boosted overall well-being more effectively than CSI, while Bucher et al.21 reported lasting improvements with ATI. HA contributed to improved QoL through consistent functional gains. Adverse effects associated with these treatments were generally mild and short-term. PRP was associated with minor, temporary pain at the injection site, while HA exhibited minimal reported side effects. BMAC and ATI were well-tolerated, with no significant complications noted. Overall, PRP and HA present promising options for managing GTPS, with ATI providing long-term benefits and BMAC showing potential that warrants further study. Additional research with larger sample sizes and standardized methods is needed to confirm these findings and compare the treatments more effectively.Discussion
This scoping review aimed to provide a comprehensive evaluation of orthobiologic treatments for GTPS, a condition that significantly affects patients’ QoL and daily functioning. Our findings suggest that orthobiologics, particularly PRP, show promise as an effective alternative to conventional therapies. PRP demonstrated promising results in reducing pain and enhancing function compared to CSI and placebo, as evidenced by improvements in key outcome measures such as the VAS score and the WOMAC. Despite these promising findings, the heterogeneity among studies and the variability in PRP formulations and administration protocols limit the generalizability of these results.The results suggest that orthobiologics, especially PRP, can effectively manage pain, improve function, and enhance QoL for patients with GTPS [Table 5]. PRP contains a high concentration of growth factors and bioactive compounds that facilitate tissue healing, reduce inflammation, and promote regeneration.1,43 When injected, these growth factors are released at the treatment site, aiding overall healing, reducing inflammation, and assisting in tendon repair.27,44,45Orthobiologics preparation and administration protocols vary widely, affecting therapeutic effects and outcomes. Various formulations, including platelet and leukocyte concentrations, activation strategies, and injection techniques influence these outcomes.19 Yan et al.46 studied the effects of Lp-PRP (Leukocyte-poor PRP) on chronic tendinopathy in rabbits, showing that Lp-PRP was more effective in treating tendinopathy and promoting tendon repair. However, Zhou et al. found that Lr-PRP impeded tendon healing due to its pro-inflammatory and catabolic effects. In addition, the strong anabolic activity of Lp-PRP may cause excessive scar tissue formation.47,48 Standardized procedures and further studies are needed to determine the optimal orthobiologic formulations and delivery methods for GTPS therapy.Orthobiologics demonstrate a favorable safety profile in the treatment of GTPS, with the majority of studies reporting only mild side effects, such as soreness or discomfort at injection site.47,49 Patients with GTPS may tolerate orthobiologics well without major side effects. However, there are limited long-term safety data, indicating that further research is needed.
PRP is the most extensively researched orthobiologic for GTPS; however BMAC, HA, and ATI are also being studied for their potential benefits in reducing pain, improving functionality, and enhancing QoL.18,19
Limitations
This review shows that orthobiologics, including PRP, BMAC, HA, and ATI may be promising for the treatment of GTPS; however there are several limitations. The studies included in this review were often small in scale and frequently lacked direct comparisons with alternative treatments such as NSAIDs or physical therapy, which limits the scope of our conclusions. Additionally, variations in the preparation and administration of PRP and CSI further complicated the ability to draw clear conclusions and apply findings broadly.
Many studies did not report whether patients had other health conditions, such as diabetes mellitus or arthritis, which could affect treatment outcomes. In addition, important lifestyle factors, including job-related stress and activity levels, were also frequently missing. Most studies only followed patients for a short period (up to six months), making it unclear if the benefits last or if further treatments are needed later on. Finally, publication bias could mean that positive results were more likely to be published, possibly skewing our findings.
Areas for Further Research
Future research on orthobiologics for GTPS should focus on developing standardized preparation and administration protocols to improve consistency in results. Comparative studies between orthobiologics and conventional treatments, such as NSAIDs or physical therapy, would help to clarify their relative benefits. Additionally, research should include patients with various comorbidities and lifestyle factors to assess how these variables impact treatment outcomes. Long-term follow-up studies are necessary to understand the enduring effects of these treatments. To create a more balanced view, studies should address publication bias by including neutral or negative findings. These steps will make the use of orthobiologics more reliable and clinically applicable.
Conclusion
The scoping review supports the use of orthobiologics, particularly PRP, as a potential treatment for GTPS. However, it emphasizes the need for further research to refine treatment protocols and establish long-term efficacy, safety, and cost-effectiveness. The review suggests that integrating orthobiologics into a multidisciplinary approach to GTPS management could improve patient outcomes, reduce disability, and enhance QoL.
Abbreviations
AUC: Area Under the Curve; AUC6: Area Under the Curve for 6 months; ATI: Autologous Tenocyte Injection; BMAC: Bone Marrow Aspirate Concentrate; CES-D: Center for Epidemiologic Studies Depression Scale; CI: Confidence Interval; CR: Case Report; CS: Case Series; CSI: Corticosteroid Injection; DN: Dry Needling; EQ-5D: EuroQol 5-Dimension; FEPS: Facial Expressions Pain Scale; FRI: Functional Rating Index; HA: Hyaluronic Acid; HHS: Harris Hip Score; HOOS: Hip disability and Osteoarthritis Outcome Score; HOS-ADL: Hip Outcome Score – Activities of Daily Living; HOS-Sport: Hip Outcome Score –
Hip Outcome Score – Sports; iHOT: International Hip Outcome Tool; iHOT-12: International Hip Outcome Tool – 12 items; iHOT-33: International Hip Outcome Tool – 33 items; LTCC: Long-Term Clinical Changes; MCID: Minimal Clinically Important Difference; MD: Mean Difference; mHHS: modified Harris Hip Score; mNPPS: modified Nirschl Pain Phase Scale; MRI: Magnetic Resonance Imaging; NASS: North American Spine Society; NR: Not Reported; NRS: Numeric Rating Scale; PASS: Patient Acceptable Symptom State; PC: Prospective Cohort; PCS: Physical Component Summary; PIS: Perceived Improvement in Symptoms; PRP: Platelet-Rich Plasma; PT: Palpatory Tenderness; QLS: Quality of Life Scores; RCT: Randomized Controlled Trial; SC: Satisfaction Score; SD: Standard Deviation; SF-36: Short Form-36; VAS: Visual Analogue Scale; VISA-G: Victorian Institute of Sport Assessment-Gluteal; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index.
Acknowledgement
N/A
Authors Contribution: Authors who Conceived and designed the analysis: Ali Parsa, Mohammad Ghorbani/ Authors who collected the data: Saeid Esmaeilian, Adam W. ANZ, Morteza Behjat/ Authors who contributed data or analysis tools: Farimah Naghibian, Neda Mirzaei, Elham Rahmanipour/ Authors who Performed the analysis: Neda Mirzaei/ Authors who Wrote the paper: All authors
Declaration of Conflict of Interest: The authors do NOT have any potential conflicts of interest for this manuscript.
Declaration of Funding: The authors received NO financial support for the preparation, research, authorship, and publication of this manuscript.
Declaration of Ethical Approval for Study: N/A
Declaration of Informed Consent: N/A
Ali Parsa MD 1,2
Saeid Esmaeilian MD, MPH 3
Adam W. Anz MD 1
Farimah Naghibian MD 4
Morteza Behjat MD 5
Neda Mirzaei PhD 2
Elham Rahmanipour MD, MPH 6
Mohammad Ghorbani MD, MPH 2
1 Andrews Institute for Orthopedics and Sports Medicine, Gulf Breeze, FL, USA
2 Orthopedic Research Center, Department of Orthopedic Surgery, Mashhad University of Medical Sciences, Mashhad, Iran
3 Department of Radiology, Shiraz University of Medical Sciences, Zand Street, Shiraz, Iran
4 Rheumatic Diseases Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
5 Department of Orthopedic Surgery, School of medicine, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran, Iran
6 Immunology Research Center, Mashhad University of Medical Sciences, Mashhad, Iran
References
- Pianka MA, Serino J, DeFroda SF, Bodendorfer BM. Greater trochanteric pain syndrome: Evaluation and management of a wide spectrum of pathology. SAGE Open Med.2021; 9:20503121211022582. doi:10.1177/20503121211022582.
- Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum.2001; 44(9):2138-45. doi:10.1002/1529 0131(200109)44:9<2138::Aid-art367>3.0.Co;2-m.
- Fearon AM, Cook JL, Scarvell JM, Neeman T, Cormick W, Smith PN. Greater trochanteric pain syndrome negatively affects work, physical activity and quality of life: a case control study. J Arthroplasty.2014; 29(2):383-6. doi:10.1016/j.arth.2012.10.016.
- Dancy ME, Alexander AS, Clark CJ, et al. Gluteal Tendinopathy: Critical Analysis Review of Current Nonoperative Treatments. JBJS Rev.2023; 11(10). doi: 10.2106/JBJS.RVW.23.00101.
- Gomez LP, Childress JM, eds. Greater Trochanteric Pain Syndrome (Greater Trochanteric Bursitis).1st Ed. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
- Lee S, Naimark M, Bedi A. Soft tissue repairs in the peri-trochanteric space. Annals of Joint. 2018; 3.
- Redmond JM, Chen AW, Domb BG. Greater Trochanteric Pain Syndrome. J Am Acad Orthop Surg. 2016; 24(4):231-40. doi:10.5435/jaaos-d-14-00406.
- Chowdhury R, Naaseri S, Lee J, Rajeswaran G. Imaging and management of greater trochanteric pain syndrome. Postgrad Med J.2014; 90(1068):576-81. doi:10.1136/postgradmedj-2013-131828.
- Torres A, Fernández-Fairen M, Sueiro-Fernández J. Greater trochanteric pain syndrome and gluteus medius and minimus tendinosis: nonsurgical treatment. Pain Manag.2018; 8(1):45-55. doi:10.2217/pmt-2017-0033.
- Rodeo SA. Orthobiologics: Current Status in 2023 and Future Outlook. J Am Acad Orthop Surg.2023; 31(12):604-613. doi:10.5435/jaaos-d-22-00808.
- Kumar A, Kadamb AG, Kadamb KG. Mesenchymal or maintenance stem cell & understanding their role in osteoarthritis of the knee joint: A review article. Arch Bone Jt Surg.2020; 8(5):560. doi: 10.22038/abjs.2020.42536.2155.
- Reid D. The management of greater trochanteric pain syndrome: A systematic literature review. J Orthop.2016; 13(1):15-28. doi:10.1016/j.jor.2015.12.006.
- Calcei JG, Rodeo SA. Orthobiologics for bone healing. Clinics in sports medicine.2019; 38(1):79-95. doi:10.1016/j.csm.2018.08.005.
- Bradsell H, Waterman B, Lansdown D, Hevesi M, Jones K, Frank RM. Incorporating Biologics Into Your Sports Medicine Practice: Who, What, When, Why, and How? Instr Course Lect.2023; 72:431-444.
- Shapiro SA, Master Z, Arthurs JR, Mautner K. Tiered approach to considering orthobiologics for patients with musculoskeletal conditions. Br J Sports Med.2023; 57(3):179-180. doi:10.1136/bjsports-2022-106494.
- Viganò M, Ragni E, Marmotti A, de Girolamo L. The effects of orthobiologics in the treatment of tendon pathologies: a systematic review of preclinical evidence. J Exp Orthop.2022; 9(1):31. doi:10.1186/s40634-022-00468-w.
- Wee J, Thevendran G. The role of orthobiologics in foot and ankle surgery: Allogenic bone grafts and bone graft substitutes. EFORT Open Rev.2017; 2(6):272-280. doi:10.1302/2058-5241.2.160044.
- Lana J, da Fonseca LF, Macedo RDR, et al. Platelet-rich plasma vs bone marrow aspirate concentrate: An overview of mechanisms of action and orthobiologic synergistic effects. World J Stem Cells.2021; 13(2):155-167. doi:10.4252/wjsc.v13i2.155.
- Pintore A, Notarfrancesco D, Zara A, et al. Intra-articular injection of bone marrow aspirate concentrate (BMAC) or adipose-derived stem cells (ADSCs) for knee osteoarthritis: a prospective comparative clinical trial. J Orthop Surg Res.2023; 18(1):350. doi:10.1186/s13018-023-03841-2.
- Pereira AA, López BM, de la Serna AR. A Comparative Study between Hyaluronic Acid and Corticosteroids for the Treatment of the Greater Trochanteric Pain Syndrome. Open Journal of Rheumatology and Autoimmune Diseases.2015; 05(03):57-61. doi:10.4236/ojra.2015.53010.
- Bucher TA, Ebert JR, Smith A, et al. Autologous Tenocyte Injection for the Treatment of Chronic Recalcitrant Gluteal Tendinopathy: A Prospective Pilot Study. Orthop J Sports Med.2017; 5(2):2325967116688866. doi:10.1177/2325967116688866.
- Vaishya R, Kumar S, Vaish A, Babu Y. Effectiveness of the guidelines for the non-operative management of knee osteoarthritis. Arch Bone Jt Surg.2021; 9(4):472-474. doi: 10.22038/abjs.2020.51112.2535.
- Moreno-Garcia A, Rodriguez-Merchan EC. Orthobiologics: current role in orthopedic surgery and traumatology. Arch Bone Jt Surg.2022; 10(7):536. doi: 10.22038/ABJS.2021.52770.2614.
- Bashkina AS, Shirokova LY, Knyazeva TS, Parulya OM, Abrosimova EB, Noskov SM. Application of platelet-rich plasma in reduction of greater trochanteric pain syndrome. Traumatology and Orthopedics of Russia. 2011; 17(2):57-61.. doi:10.21823/2311-2905-2011-0-2-57-61.
- Begkas D, Chatzopoulos ST, Touzopoulos P, Balanika A, Pastroudis A. Ultrasound-guided Platelet-rich Plasma Application Versus Corticosteroid Injections for the Treatment of Greater Trochanteric Pain Syndrome: A Prospective Controlled Randomized Comparative Clinical Study. Cureus.2020; 12(1):e6583. doi:10.7759/cureus.6583.
- RR M. Abstracts from the 12th Congress of the European Hip Society. Hip Int.2016; 26 Suppl 2(2_suppl):3-92. doi:10.5301/hipint.5000450.
- Shirokova K, Noskov S, Shirokova L, Gorokhova V. Platelet-rich plasma treatment in patients with osteoarthritis of the hip and greater trochanteric pain syndrome. Osteoarthritis and Cartilage.2018; 26:S144. doi:10.1016/j.joca.2018.02.312.
- Ribeiro AG, Ricioli WJ, Silva AR, Polesello GC, Guimarães RP. Prp in the Treatment of Trochanteric Syndrome: A Pilot Study. Acta Ortop Bras.2016; 24(4):208-212. doi:10.1590/1413-785220162404159837.
- Oderuth E, Ali M, Atchia I, Malviya A. A double blind randomised control trial investigating the efficacy of platelet rich plasma versus placebo for the treatment of greater trochanteric pain syndrome (the HIPPO trial): a protocol for a randomised clinical trial. Trials.2018; 19(1):517. doi:10.1186/s13063-018-2907-x.
- Thompson G, Pearson JF. No attributable effects of PRP on greater trochanteric pain syndrome. N Z Med J.2019; 132(1507):22-32.
- Jacobson JA, Yablon CM, Henning PT, et al. Greater Trochanteric Pain Syndrome: Percutaneous Tendon Fenestration versus Platelet-Rich Plasma Injection for Treatment of Gluteal Tendinosis. J Ultrasound Med.2016; 35(11):2413-2420. doi:10.7863/ultra.15.11046.
- Blucher N, Nahas S, Bonatsos V, Patel A, Sarraf K, Vedi V. Platelet-rich-plasma injections for the treatment of resistant trochanteric pain. International Journal of Surgery.2016; 36:S32. doi:10.1016/j.ijsu.2016.08.044.
- Massimi S, LaSalle E, Vongvorachoti J, Lutz GE. Ultrasound-Guided Platelet Rich Plasma (PRP) Injections for Greater Trochanteric Pain Syndrome (GTPS): A Retrospective Case Series. Pm&R.2013; 5(9S):S206-S207. doi:10.1016/j.pmrj.2013.08.298.
- Mautner K, Colberg RE, Malanga G, et al. Outcomes after ultrasound-guided platelet-rich plasma injections for chronic tendinopathy: a multicenter, retrospective review. PM&R. 2013; 5(3):169-75. doi:10.1016/j.pmrj.2012.12.010.
- Unlu MC, Kivrak A, Kayaalp ME, Birsel O, Akgun I. Peritendinous injection of platelet-rich plasma to treat tendinopathy: A retrospective review. Acta Orthop Traumatol Turc.2017; 51(6):482-487. doi:10.1016/j.aott.2017.10.003.
- Hegarty DA. Abstracts of the 10th World Congress of the World Institute of Pain (WIP), 26-29 August, 2020, Rome Marriott Park Hotel – Rome. Pain Pract.2020;20 Suppl 1(S1):7-103. doi:10.1111/papr.12886.
- Rajeev A, Yiannis S, Rajpal-Singh K. Abstracts from the 12th Congress of the European Hip Society. Hip Int.2016; 26 Suppl 2(2_suppl):3-92. doi:10.5301/hipint.5000450.
- Gorelick L, Rozano-Gorelick A, Robinson D, Marcus O, Joubran S, Ram E. Treatment of Hip Trochanteric Bursitis Using Hyaluronate Injections. Open Journal of Rheumatology and Autoimmune Diseases.2013; 03(02):125-129.doi:10.4236/ojra.2013.32019.
- Pereira AA, López BM, de la Serna AR. A Comparative Study between Hyaluronic Acid and Corticosteroids for the Treatment of the Greater Trochanteric Pain Syndrome. Open Journal of Rheumatology and Autoimmune Diseases.2015; 5(03):57.
- Henderson RG, Colberg RE. Pure bone marrow aspirate injection for chronic greater trochanteric pain syndrome: a case report. Pain Manag.2018; 8(4):271-275. doi:10.2217/pmt-2018-0008.
- Fitzpatrick J, Bulsara MK, O’Donnell J, McCrory PR, Zheng MH. The Effectiveness of Platelet-Rich Plasma Injections in Gluteal Tendinopathy: A Randomized, Double-Blind Controlled Trial Comparing a Single Platelet-Rich Plasma Injection With a Single Corticosteroid Injection. Am J Sports Med.2018; 46(4):933-939. doi:10.1177/0363546517745525.
- Lee JJ, Harrison JR, Boachie-Adjei K, Vargas E, Moley PJ. Platelet-Rich Plasma Injections with Needle Tenotomy for Gluteus Medius Tendinopathy: A Registry Study with Prospective Follow-up. Orthop J Sports Med.2016; 4(11):2325967116671692. doi:10.1177/2325967116671692.
- Walker-Santiago R, Wojnowski NM, Lall AC, Maldonado DR, Rabe SM, Domb BG. Platelet-Rich Plasma Versus Surgery for the Management of Recalcitrant Greater Trochanteric Pain Syndrome: A Systematic Review. Arthroscopy.2020; 36(3):875-888. doi:10.1016/j.arthro.2019.09.044.
- Fitzpatrick J, Bulsara M, Zheng MH. The Effectiveness of Platelet-Rich Plasma in the Treatment of Tendinopathy: A Meta-analysis of Randomized Controlled Clinical Trials. Am J Sports Med.2017; 45(1):226-233. doi:10.1177/0363546516643716.
- Migliorini F, Kader N, Eschweiler J, Tingart M, Maffulli N. Platelet-rich plasma versus steroids injections for greater trochanter pain syndrome: a systematic review and meta-analysis. Br Med Bull.2021; 139(1):86-99. doi:10.1093/bmb/ldab018.
- Yan R, Gu Y, Ran J, et al. Intratendon Delivery of Leukocyte-Poor Platelet-Rich Plasma Improves Healing Compared With Leukocyte-Rich Platelet-Rich Plasma in a Rabbit Achilles Tendinopathy Model. Am J Sports Med.2017; 45(8):1909-1920. doi:10.1177/0363546517694357.
- Ali M, Oderuth E, Atchia I, Malviya A. The use of platelet-rich plasma in the treatment of greater trochanteric pain syndrome: a systematic literature review. J Hip Preserv Surg.2018; 5(3):209-219. doi:10.1093/jhps/hny027.
- Zhou Y, Zhang J, Wu H, Hogan MV, Wang JH. The differential effects of leukocyte-containing and pure platelet-rich plasma (PRP) on tendon stem/progenitor cells – implications of PRP application for the clinical treatment of tendon injuries. Stem Cell Res Ther.2015; 6(1):173. doi:10.1186/s13287-015-0172-4.
- Boyd M, Vijayaraghavan N, Karvelas K. Evidenced-Based Management of Greater Trochanteric Pain Syndrome. Current Physical Medicine and Rehabilitation Reports.2020; 8(4):313-321. doi:10.1007/s40141-020-00294-0.


