

Background:
Avulsion of the biceps femoris from the fibula and proximal tibia is encountered in clinical practice. While the anatomy of the primary posterolateral corner structures has been qualitatively and quantitatively described, a quantitative analysis regarding the insertions of the biceps femoris on the fibula and proximal tibia is lacking.Purpose:
To quantitatively assess the insertions of the biceps femoris, fibular collateral ligament (FCL), and anterolateral ligament (ALL) on the fibula and proximal tibia as well as establish relationships among these structures and to pertinent surgical anatomy.Study Design:
Descriptive laboratory study.Methods:
Dissections were performed on 12 nonpaired, fresh-frozen cadaveric specimens identifying the biceps femoris, FCL, and ALL, and their insertions on the proximal tibia and fibula. The footprint areas, orientations, and distances from relevant osseous landmarks were measured using a 3-dimensional coordinate measurement device.Results:
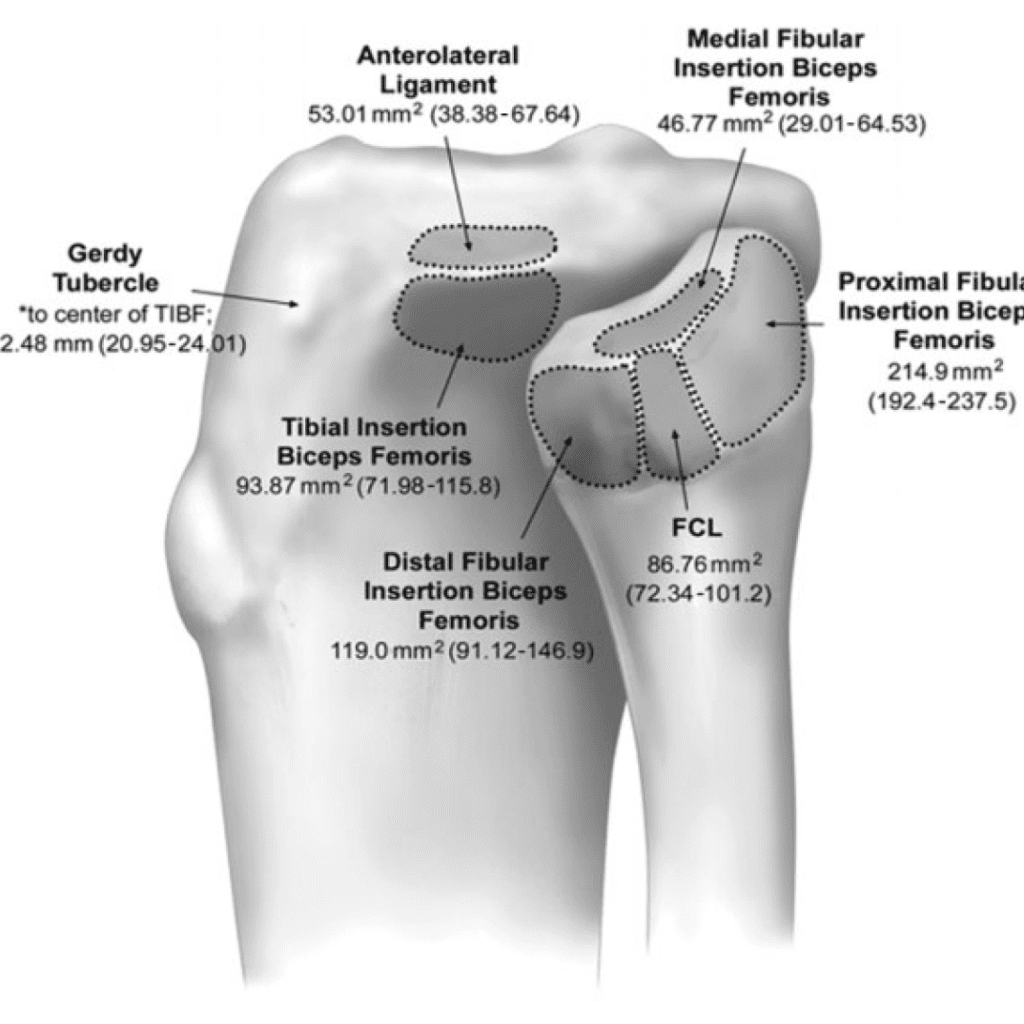
Dissection produced 6 easily identifiable and reproducible anatomic footprints. Tibial footprints included the insertion of the ALL and an insertion of the biceps femoris (TBF). Fibular footprints included the insertion of the FCL, a distal insertion of the biceps femoris (DBF), a medial footprint of the biceps femoris (MBF), and a proximal footprint of the biceps femoris (PBF). The mean area of these footprints (95% CI) was as follows: ALL, 53.0 mm2 (38.4-67.6); TBF, 93.9 mm2 (72.0- 115.8); FCL, 86.8 mm2 (72.3-101.2); DBF, 119 mm2 (91.1-146.9); MBF, 46.8 mm2 (29.0-64.5); and PBF, 215 mm2 (192.4- 237.5). The mean distance (95% CI) from the Gerdy tubercle to the center of the ALL footprint was 24.3 mm (21.6-27.0) and to the center of the TBF was 22.5 mm (21.0-24.0). The center of the DBF was 8.68 mm (7.0-10.3) from the anterior border of the fibula, the center of the FCL was 14.6 mm (12.5-16.7) from the anterior border of the fibula and 20.7 mm (19.0-22.4) from the tip of the fibular styloid, and the center of the PBF was 8.96 mm (8.2-9.7) from the tip of the fibular styloid.Conclusion:
A tibial footprint, distal fibular footprint, medial fibular footprint, and proximal fibular footprint were all consistent components of the insertion of the biceps femoris. Consistent relationships existed between the biceps femoris and insertions of the ALL and FCL.Clinical Relevance:
The size of these footprints and distances from pertinent surgical landmarks will guide repairs of biceps femoris avulsion injuries.Keywords:
biceps femoris; fibular collateral ligament; avulsion; anterolateral ligament; repairIntroduction
Avulsion injury of the distal biceps femoris can occur as an isolated injury or as part of a multiligament injury pattern, with or without concomitant injury to additional lateral knee structures. ‖Through qualitative, quantitative, and biomechanical study, the anatomy and strength of the fibular collateral ligament (FCL), popliteofibular ligament, and popliteus tendon have been described thoroughly.2,9,14,20 While the anatomy of the biceps femoris has also been qualitatively described,7,10,12,19,20,22 a quantitative analysis of its tendinous insertions on the fibula and proximal tibia is lacking.Previous qualitative description of the biceps femoris has elicited fascial and tendinous components of both the long head and the short head.7,10,12,18-22 The descriptions by Terry and LaPrade19 of the tendinous components of the long head included a direct arm, which inserts on the posterolateral aspect of the proximal fibula lateral to the styloid, and an anterior arm, in which insertion starts along the lateral edge of the proximal fibula lateral to FCL and continues distally to end in an anterior aponeurosis overlying the anterior compartment of the leg. Description of the tendinous components of the short head included a direct arm, which inserts just lateral to the fibular styloid and medial to the FCL, and an anterior arm, whose insertion begins medial to the FCL and continues anteriorly blending with the anterior tibiofibular ligament, with additional insertions continuing to the lateral tibia 1 cm posterior to the Gerdy tubercle. 19 Another qualitative description by Tubbs et al22 described a split of the biceps femoris insertion by the FCL into a medial slip and a lateral slip, with both components contiguous at their attachment site into the fibular head. The fibers anterior and posterior to the FCL convalesced to form a ring around the FCL, which tightened on traction of the tendon.The purpose of this study was to provide quantitative information regarding the tendinous insertions of the biceps femoris upon the proximal fibula and tibia, as repair of these structures often constitutes the goal of surgical treatment of avulsion injury. It was hypothesized that for the biceps femoris, there would be consistent relationships with pertinent osseous landmarks and the distal insertions of the FCL and anterolateral ligament (ALL). A comprehensive understanding of the anatomical attachment sites of the biceps femoris, FCL, and ALL will assist in guiding biceps femoris surgical repair and reconstruction techniques.Methods
Specimen Preparation Twelve nonpaired, fresh-frozen cadaveric specimens (7 female, 5 male) with a mean age of 61.3 years (range, 53-66 years), mean height of 1.69 m (range, 1.55-1.78 m), mean weight of 93.58 kg (range, 45.36-127.0 kg), and mean body mass index (BMI) 33.2 kg/m2 (range, 16-47 kg/m2) without history of injury were used in the study. We selected 12 specimens per group, as 10 and 12 specimens has proven a sufficient sample size in previous quantitative studies on ligamentous anatomy.3,9 The knees were disarticulated, with obstructing soft tissue, ligaments, and tendons removed, including the femur and proximal musculature. Clear identification of the biceps femoris, FCL, and ALL, and their insertions upon the proximal tibia and fibula was performed. The tibia and fibula were fixed in cylindrical PVC pipe using automotive body filler (Bondo; 3M). The specimen was then clamped to a custom support structure, ensuring a constant and fixed spatial relationship to the measuring device throughout data capture. The ligamentous attachment centers of each structure were identified on the basis of their distinct insertions and were marked with a surgical marking pen (Figure 1).Anatomic Measurements
Three-dimensional positional data were collected using a calibrated stylus utilizing standard system software (MicroScribe Utility Software; Revware Inc) that measured interspatial relationships between reference points (Figure 2). All data were captured by the senior author (A.W.A.). Data postprocessing was accomplished utilizing numerical computation software (MATLAB R2014b). For accurate measurement of the ligament and tendon footprints, immediately prior to data capture, the individual structures were tagged with sutures, removed from their proximal origin, and then sharply dissected off of their distal footprint to clearly identify their attachments. The periphery of each footprint was measured with points collected at 1-mm increments. Data points of pertinent osseous landmarks were also collected. From these points, the ligament attachment centers, distances to osseous prominences, and ligament footprint areas were calculated. Principal component analysis was used to reduce the dimensionality, allowing for plane fitting and 2-dimensional calculations of area. A point-inclusion algorithm was used to remove any points that were internal to the points defined by the outer polygon. Using the Heron formula, areas were calculated on the reduced 2-dimensional data set in an iterative process around the vertices set. Centroids were subsequently translated back to 3 dimensions and coordinated for linear comparison between landmarks. Data reduction and area calculation techniques were similar to those used by Brinkman et al2 in a previous quantitative study on the posterolateral corner. All reported measurements were performed by the same individual, with guidance by the senior author (A.W.A.) to eliminate interobserver variability.System Validation
To assess the accuracy of the measuring device, a single-point articulation performance test (SPAT) was performed based on the B89.4 22 American Society of Mechanical Engineers (ASME) standard and the manufacturer’s recommendations. The average SPAT result was 0.01 mm. The SPAT reflects both the repeatability and reproducibility of measurements using this device in our laboratory testing environment. Therefore, values <0.01 mm may be attributed to error within the measurement system, and values >0.01 mm may be considered significant.Results
The tendinous portions of the long head and short head of the biceps were readily identifiable proximal to the insertion. Proximal to the fibula, the tendons of the long and short head coalesced, with some individual fibers continuing discretely from each muscle belly. The coalesced tendon began its insertion upon the fibula proximally and was split by the FCL as the insertion continued distally. Four easily identifiable and reproducible anatomic tendinous footprints were encountered: a proximal footprint of the biceps femoris upon the fibula (PBF) composed of fibers from both the short head and the long head, a distal lateral insertion of the biceps femoris upon the fibula (DBF) composed predominantly of fibers from the long head, a medial footprint of the biceps femoris upon the fibula (MBF) composed predominantly of fibers from the short head, and an insertion of the biceps femoris upon the tibia with a variable composition of fibers composed either predominantly from the long head or from the short head or a combination of the two. Footprint areas are presented in Figure 3, and distance from the center of the footprint areas to the surgical anatomic landmarks are presented in Table 1. The FCL and ALL were identifiable and distinct in all 12 specimens.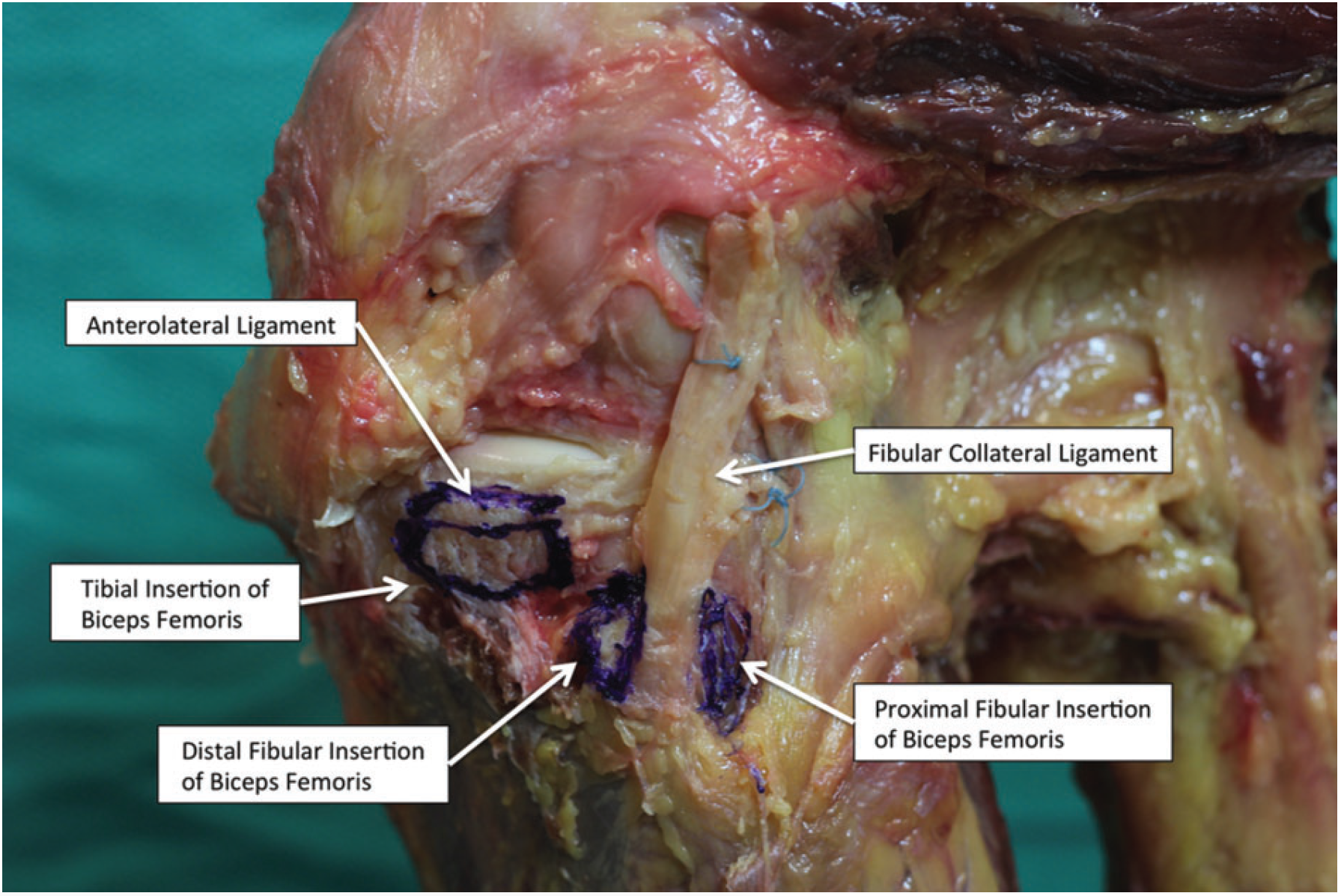
Figure 1. Dissection illustrating the anatomic structure.
Figure 2. MicroScribe setup.
Discussion
The purpose of this study was to quantitatively analyze the insertion of the biceps femoris to better guide repair in the setting of avulsion injury. We found 4 distinct footprint insertions of the biceps femoris, including a large footprint upon the tibia. Additionally, we found consistent relationships to the FCL, ALL, and pertinent surgical landmarks. This study quantitatively captures the broadness and complexity of the insertional area of the biceps femoris, illustrating its relationship with the surrounding lateral structures. This raises questions concerning the optimal method of repair. The broad fibular insertion of the biceps femoris has guided our clinical practice to place 1 suture anchor at the proximal footprint and 1 suture anchor at the distal footprint. Additionally, the robustness of the tibial insertion has guided our clinical practice to include an additional suture anchor upon the tibia. Considering the size of the footprint, we theorize that a double-row style repair, similar to that employed in shoulder surgery, may provide a stronger, more anatomic repair.The qualitative findings in this study are similar to those of Terry and LaPrade19 regarding the biceps complex. Their description of the tendinous insertions involved a direct and anterior arm for the long head and a direct and anterior arm for the short head. While our dissection produced similar findings when determining the insertion footprints, we found it more difficult to discriminate between what they described as the direct head of the long head and the direct head of the short head. On our dissection, the short head and long head produced a confluence that inserted onto the proximal fibular head, which we termed the proximal fibular insertion of the biceps femoris. Similarly to the description by Terry and LaPrade19 of the anterior band of the long head of the biceps, we found that the fibers compromising the distal footprint of the biceps femoris upon the fibula were composed of bands from the long head, with fibers continuing to form a confluence with the fascia of the anterior compartment of the leg.Also, similar to their description, we found a footprint medial to the FCL composed essentially of fibers from the short head that also extended anteriorly, blending with the capsule of the proximal tibiofibular joint. However, we found variability regarding the distal termination of both the long head and short head—what previously has been described as the anterior bands of the long head and the short head. We consistently found an insertion of the biceps upon the tibia similar to previous studies, which we termed the tibial footprint of the biceps femoris (TBF). This has been described as a termination of the anterior band of the short head by Terry and LaPrade19 or described as a confluence of continuing fibers split by the FCL as described by Tubbs et al.22 In our dissections, we found variability in the composition of this insertion. At times, the insertion was composed predominantly of fibers from the long head, predominantly of fibers from the short head, and fibers from both the long head and the short head.
Regarding distances to pertinent osseous landmarks, we found some similarities and some dissimilarities to previous studies. This study determined the distance between the Gerdy tubercle and the TBF to be 22.5 mm (95% CI, 21.0-24.0). The tendinous insertion of the anterior arm of the short head of the biceps femoris was reported by Terry and LaPrade19 to be 1 cm posterior to the Gerdy tubercle. We found an insertion center of the FCL to be 14.6mmfrom the anterior border of the fibula and 20.7mm from the tip of the styloid. Previous quantitative analysis of the FCL has measured the distance from the distal FCL to the anterior border of the fibula to be 8.2 mm and the tip of the styloid as 28.4 mm.9
This study determined the area of the fibular insertion of the FCL to be 86.8 mm2 (95% CI, 72.3-101.2); previous studies2,9 have reported this area to be 43 mm2 and 35 mm2. Variation between our study findings and previous analyses may be attributed to the size of the anatomic specimens as well as the methods of measurement. Previous anatomic study of the biceps femoris did not report the age, weight, height, or BMI of their specimens, nor was the exact method made for measurements reported. The previous anatomic study of the posterolateral corner by LaPrade et al9 used a video motion analysis measurement system utilizing a fine marker and infrared technology; while age was reported in this study, height, weight, and BMI were not. Our tendency was to err on the side of capturing all potential fibers that appeared functional regarding the measured structures.
| Landmark | Distance, mm |
|---|---|
| Gerdy tubercle to ALL | 24.3 (21.6-27.0) |
| Gerdy tubercle to TBF | 22.5 (21.0-24.0) |
| DBF to anterior border, fibula | 8.68 (7.0-10.3) |
| FCL to anterior border, fibula | 14.6 (12.5-16.7) |
| FCL to tip of fibula, styloid | 20.7 (19.0-22.4) |
| PBF to tip of fibula, styloid | 8.96 (8.2-9.7) |
| aValues are expressed as mean (95% CI). ALL, anterolateral ligament; DBF, distal fibular insertion of the biceps femoris; FCL, fibular collateral ligament; PBF, proximal fibular insertion of the biceps femoris; TBF, tibial footprint of the biceps femoris. | |
One weakness of this study is that it focused on the tendinous insertions of the biceps femoris while fascial components of the biceps femoris were not quantitatively evaluated. Additionally, the variability of which the head predominantly contributed to a determined footprint could have been captured in a more quantifiable fashion. The sample number may not have captured a full demographic, although our sample number was similar to previous recent anatomic studies utilizing similar measuring technology.3,9
Conclusions
A tibial footprint, distal fibular footprint, medial fibular footprint, and proximal fibular footprint were all consistent components of the insertion of the biceps femoris. Consistent relationships existed between the biceps femoris and insertions of the ALL and the FCL. The size of these footprints and distances from pertinent surgical landmarks will guide the placement of repairs and reconstructions of lateral knee injury.References
1. Alioto RJ, Browne JE, Barnthouse CD, Scott AR. Complete rupture of the distal semimembranosus complex in a professional athlete. Clin Orthop Relat Res. 1997;336:162-165.2. Brinkman JM, Schwering PJ, Blankevoot L, Kooloos JG, Luites J, Wymenga A. The insertion geometry of the posterolateral corner of the knee. J Bone Joint Surg Br. 2005;87:1364-1368.
3. Campbell KJ, Michalski MP, Wilson KJ, et al. The ligament anatomy of the deltoid complex of the ankle: a qualitative and quantitative anatomical study. J Bone Joint Surg Am. 2014;96:e62.
4. David A, Buchholz J, Muhr G. Tear of the biceps femoris tendon. Arch Orthop Trauma Surg. 1994;113:351-352.
5. Fortems Y, Victor J, Dauwe D, Fabry G. Isolated complete rupture of biceps femoris tendon. Injury. 1995;26:275-276.
6. Jensen IH, Kramhoft M. Distal rupture of the biceps femoris muscle. Scand J Med Sci Sports. 1994;4:259-260.
7. Kaplan EB. The iliotibial tract: clinical and morphological significance. J Bone Joint Surg. 1958;40:817-832.
8. Kusma M, Seil R, Kohn D. Isolated avulsion of the biceps femoris insertion-injury patterns and treatment options: a case report and literature review. Arch Orthop Trauma Surg. 2007;127:777-780.
9. LaPrade RF, Ly TV, Wentorf FA, Engebretsen L. The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med. 2003;31:854-860.
10. Last RJ. Some anatomical details of the knee joint. J Bone Joint Surg Br. 1948;30B:683-688.
11. Lempainen L, Sarimo J, Mattila K, Heikkila J, Orava S, Puddu G. Distal tears of the hamstring muscles: review of the literature and our results of surgical treatment. Br J Sports Med. 2007;41:80-83.
12. Marshall JL, Girgis FG, Zelko RR. The biceps femoris tendon and its functional significance. J Bone Joint Surg. 1972;54:1444-1450.
13. McGoldrick F, Colville J. Spontaneous rupture of biceps femoris. Arch Orthop Trauma Surg. 1990;109:234.
14. Moorman CT, LaPrade RF. Anatomy and biomechanics of the posterolateral corner of the knee. J Knee Surg. 2005;18:137-145.
15. Pan KL, Ting F. Delayed repair of rupture of the biceps femoris tendon— a case report. Med J Malaysia. 2000;55:368-370.
16. Schilders E, Bismil Q, Sidhom S, Robinson P, Barwick T, Talbot C. Partial rupture of the distal semitendinosus tendon treated by tenotomy— a previously undescribed entity. Knee. 2006;13:45-47.
17. Sebastianelli WJ, Hanks GA, Kalenak A. Isolated avulsion of the biceps femoris insertion. A case report. Clin Orthop Relat Res. 1990;259:200-203.
18. Terry GC, Hughston JC, Norwood LA. The anatomy of the iliopatellar band and iliotibial tract. Am J Sports Med. 1986;14:39-45.
19. Terry GC, LaPrade RF. The biceps femoris muscle complex at the knee: its anatomy and injury patterns associated with acute anterolateral-anteromedial rotatory instability. Am J Sports Med. 1996;24:2-8.
20. Terry GC, LaPrade RF. The posterolateral aspect of the knee. Anatomy and surgical approach. Am J Sports Med. 1996;24: 732-739.
21. Terry GC, Norwood LA, Hughston JC, Caldwell KM. How iliotibial tract injuries of the knee combine with acute anterior cruciate ligament tears to influence abnormal anterior tibial displacement. Am J Sports Med. 1993;21:55-60.
22. Tubbs RS, Caycedo FJ, Oakes WJ, Salter EG. Descriptive anatomy of the insertion of the biceps femoris muscle. Clin Anat. 2006;19: 517-521.
23. Valente M, Mancuso F, Alecci V. Isolated rupture of biceps femoris tendon. Musculoskelet Surg. 2013;97:263-266.
24. Verburgh H, Keeman JN. Complete ruptuur van de M biceps femorispees. Ned Tijdschr Geneesk. 1991;135:1970-1971.
25. Werlich T. Isolated rupture of the biceps tendon of the knee joint [in German]. Unfallchirurg. 2001;104:187-190.
The Orthopaedic Journal of Sports Medicine, 3(9), 2325967115602255 DOI: 10.1177/2325967115602255 ª The Author(s) 2015
This open-access article is published and distributed under the Creative Commons Attribution – NonCommercial – No Derivatives License (http://creativecommons.org/ licenses/by-nc-nd/3.0/), which permits the noncommercial use, distribution, and reproduction of the article in any medium, provided the original author and source are credited. You may not alter, transform, or build upon this article without the permission of the Author(s). For reprints and permission queries, please visit SAGE’s Web site at http://www.sagepub.com/journalsPermissions.nav.For additional information on ACL knee injuries, or to learn more about what is involved during ACL reconstruction surgery, please contact the office of orthopedic knee surgeon, Dr. Adam Anz, serving the greater Pensacola, Gulf Breeze, and Gulf Coast communities.


