

The menisci are c-shaped, rubber-like cartilage discs that reside inside the knee joint. There are two menisci in every knee, one on the inner side (medial meniscus) and one on the outer side (lateral meniscus). Their function is to increase surface area for weight transmission between the cartilage on the ends of the bone, which decreases pressure between the ends of the bone and adds to stability of the joint. Both the medial and lateral menisci have stout attachments at the front and back of the tibia, these attachments are often called “roots”. These meniscal roots are important because they hold the meniscus in place to provide stability to the entire meniscus. The stability is obtained by a functional circumferential hoop which the C-shape obtains with attaching at the roots. This functional hoop stability prevents the meniscus from extruding out when pressure is exerted across the joint, effectively keeping the meniscus in place between the two bones.
Meniscus tears can occur in a number of different shapes and scenarios. They can occur as a result of accumulative wear and tear of the joint or as the result of an injury. Sometimes, wear and tear changes in the meniscus can be subtle until an injury event occurs and the scenario is worsened drastically. Tears of the meniscus root are especially concerning because they compromise the functional hoop property of the meniscus, rendering the meniscus non-functional. When there is a tear of the meniscal root the studies have suggested that pressure upon the cartilage is increased to levels similar to having no meniscus at all. This can subsequently cause early degeneration of the joint.
Meniscus root tears are often seen in two groups of patients:
The primary symptoms of a meniscus root tear include pain on the inside or outside of the knee with mechanical symptoms. Certain activities such as pivoting, running, climbing, or even getting up from a chair may produce symptoms including popping and catching. Patients may hear or feel a clicking sound with movement, and the knee may be tender to the touch for some in specific locations.
Figure 1, Coronal view of normal meniscal root
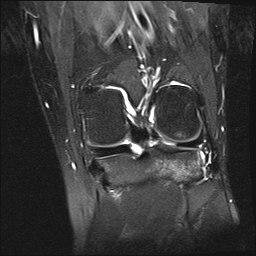
While an X-ray will not show meniscal damage, it is necessary to evaluate the overall health of the knee joint, as subtle changes on X-rays are common and help to guide treatment. Although a history, physical exam and x-ray are important in diagnosis, an MRI is important to visualize the meniscal root (Figure 1). These root tears can be very difficult to identify on MRI but is most often diagnosed when a “ghost sign” is seen. Meniscal root tears can be seen on coronal, axial and sagittal MRI views. On the sagittal view, as seen in figure 3, there is a ghost sign which is indicative of a meniscal root tear. A normal, healthy meniscus should look like a dark black triangle. On the coronal view, as seen in figure 2, there is a tear of the meniscal root.

Figure 2, Coronal View with “Ghost Sign”
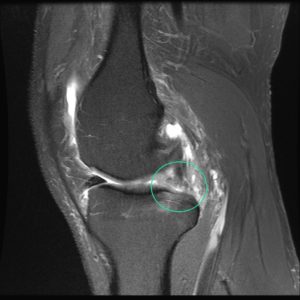
Figure 3, Sagittal View with “Ghost Sign”
Treatment of meniscal root tears can be very difficult, especially in older patients. In older patients, repair can be difficult as tears are not commonly diagnosed until progression of arthritis is more severe. In younger patients, repair is much easier due to decreased prevalence of joint degeneration.

Figure 4, Normal Meniscal Root
An arthroscopic approach is utilized to repair the meniscal root. Once access is made into the knee, Dr. Anz will visualize the meniscal root (Figure 4). A device is used to pull on the root to confirm the presence of a tear. After a tear is confirmed, Dr. Anz will use a guide to drill a tunnel at the anatomic site of the original root. (Figure 5) This tunnel will become the new home for the torn meniscal root. Sutures will be passed through the torn portion (Figure 6) of the meniscus and shuttled down into the tunnel previously drilled. Once the sutures have been pulled into the tunnel, Dr. Anz will visualize the meniscus and tighten the sutures and secure them with a suture anchor.
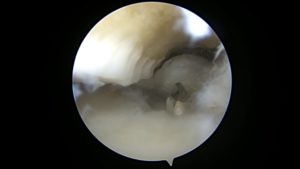
Figure 5, Drill bit coming up from root attachment

Figure 6, Sutures passed through the root repair
After surgery, the patient will be non-weight bearing for 6 weeks to allow for healing of the repair. Physical therapy may be initiated the day after surgery. Range of motion at the knee is limited to 90 degrees of flexion for the first weeks in order to prevent excess stress on the repair. Six weeks after surgery a partial protective weight bearing program is initiated to slowly wean from the crutches. Patients should avoid impact activities, deep squats, and lifting in a deep squat for a minimum of 4 months after surgery to protect the meniscus root repair.
For more information on meniscus injuries, or to learn more about the surgical treatments for meniscus tears offered by Dr. Adam Anz, Orthopedic Surgeon/Sports Medicine Specialist, please contact our office.
[social_warfare buttons=”facebook,twitter”]
A biomechanical study that we completed at the Andrews Research and Education Foundation was published in the American Journal of Sports Medicine.
The study evaluated the repair strengths of four meniscus repair methods for radial meniscus tears. Radial meniscus tears can accompany anterior cruciate ligament (ACL) tears, particularly radial tears of the lateral meniscus. A new instrument known as the Ceterix Novostitch was evaluated.
The study determined that complex patterns of suture repair are stronger than simple patterns.
To read the full study click here.
Meniscus is a very important part of the knee joint. It is a type of cartilage that serves as a shock absorber within the knee since very high loads are transmitted across the knee with walking, running, jumping, going up and down stairs, or participating in sports or other active extracurricular activities. The menisci are c-shaped pieces of cartilage that cover the knee and are extremely important to distribute the load across the knee and protect the articular cartilage. The menisci also serve as secondary stabilizers to the knee to assist the ligaments.
The knee needs the meniscus in order to function. If a meniscus sustains a significant tear, it loses its ability to function. Over time this will lead to degradation and wear of the articular cartilage, called arthritis. This eventually can lead to osteoarthritis and bring a myriad of unwanted symptoms.
The symptoms of a meniscus tear include pain on the inside or outside of the knee, a feeling of instability, locking, catching, and tenderness. An MRI will be used to confirm a meniscus injury. If the meniscus shows a small tear, the patient may be able to heal without surgery by way of physical therapy. For larger tears, those that have failed non-operative management, and those with frank mechanical symptoms surgery is typically recommended.
A meniscectomy will be performed on the knee if the meniscus has a small symptomatic tear, one that is shredded beyond repair, or a tear in the inner third of the meniscus. This procedure essentially removes the area of the tear, and removes the damaged section. This is called a partial meniscectomy. Dr. Anz will take great care to only remove the damaged part of the tear and leave as much of the healthy meniscus as possible.
For tears that occur in the outer two thirds of the meniscus, or for larger tears that can be fixed, an attempt is made to repair the meniscus and preserve as much of the native meniscus as possible. This is performed with a combination arthroscopic and open procedure. Strong stitches are placed through the tear to bring the tissue back together and complete the repair.
After a meniscal repair, the knee must be protected to allow the meniscus to heal. For a partial meniscectomy procedure, the patient is allowed to weight-bear as tolerated. Physical therapy is started immediately to regain motion and strength. Weight bearing is protected on crutches for two weeks followed by full weight bearing in the brace, which is worn for a total of six weeks.
To learn more about mensical injuries of the knee, or for additional information on meniscus repairs or meniscus surgery of the knee, please contact the Gulf Breeze, Florida orthopedic surgeon, Dr. Adam Anz located at the Andrews Institute.
