
The PCL (posterior cruciate ligament) is a ligament that is located inside the knee joint near the back of the knee.
This particular ligament is responsible for keeping the bone in the leg from moving backward (or posterior) in relation to the bone in the thigh. A PCL can become damaged or injured through sports or other traumatic accident such a motor vehicle collision. Some of these injuries may present themselves as mild tears, while others represent full tears. PCL knee injuries are not as common as ACL knee injuries, however, many times it is because a PCL knee injury may simply go undiagnosed.
Mild PCL knee injuries can oftentimes heal on their own. In certain instances the ligament is torn to the extent that a PCL reconstruction may be necessary.
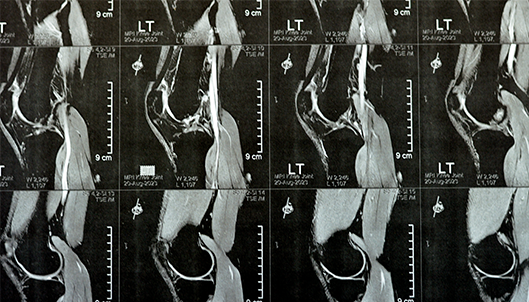
Dr. Anz performs PCL knee reconstructions following a thorough assessment of the knee using an MRI so that the extent of the injury, location, and pattern of injury can be determined.
Surgical reconstruction of the PCL is usually only recommended for grade III PCL tears. During a PCL reconstruction, Dr. Anz will reconstruct the ligament using a graft. This graft usually consists of donated tissue (i.e. the quadriceps) from another person (known as an allograft). Sutures will be used to complete this process and to tightly secure the ligament to as close to its native footprint as possible.

Following PCL reconstruction surgery, a brace is required for six months to prevent gravity from stretching out the reconstructed ligament. Physical therapy is a very important part of the recovery process and is recommended in order for the patient to make a full recovery and receive optimal results. It is recommended, that after surgery, rehabilitation begin so that patients can begin striving towards range of motion, strengthening of the knee, and full mobility. Initially, patients cannot place weight on their leg for 6 weeks. Strengthening begins at seven weeks, and running and cutting sports are delayed for up to 24 months.
—
For additional information on ligament injuries of the knee, or to learn more about PCL reconstruction surgery of the knee, please contact the Gulf Breeze, Florida orthopedic surgeon, Dr. Adam Anz located at the Andrews Institute.